Originally published on Ultrasound G.E.L. on 9/3/18 – Visit HERE to listen to accompanying PODCAST! Reposted with permission.
Follow Dr. Michael Prats, MD (@PratsEM), Dr. Creagh Bougler, MD (@CreaghB), and Dr. Jacob Avila, MD (@UltrasoundMD) from Ultrasound G.E.L. team!

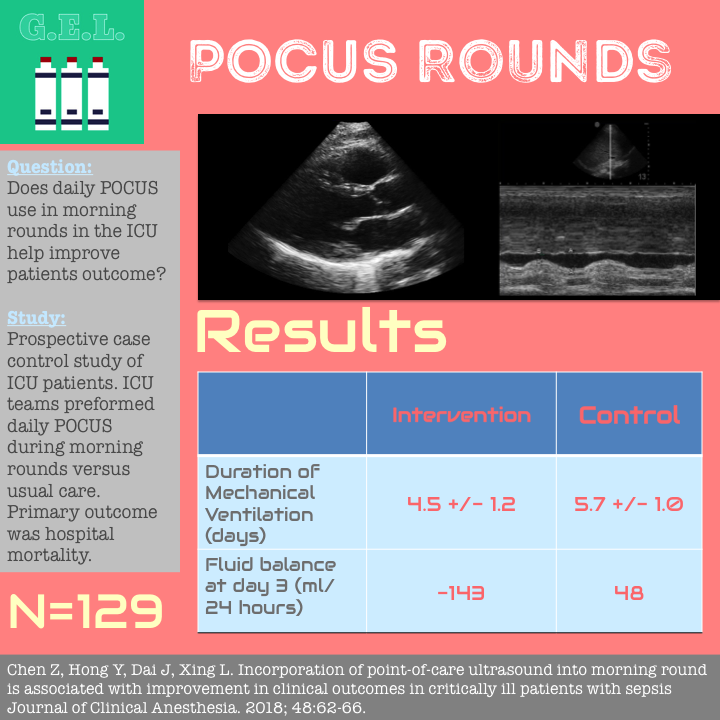
Incorporation of point-of-care ultrasound into morning roond is associated with improvement in clinical outcomes in critically ill patients with sepsis
Journal of Clinical Anesthesia May 2018 – Pubmed Link
Take Home Points
1. Protocolized daily US rounds in the ICU may lead to modest improvements in outcomes such as length of stay and duration of mechanical ventilation.
2. Larger studies are needed to confirm these results, determine if mortality benefit, and suggest the mechanism for these benefits.
Background
We know that severe/sepsis and/or septic shock are bad and those with either are at increased risk of death. We also know the POCUS use is increasing in the ICU and can be helpful in obtaining information to aid in medical decision making. Most trials using ultrasound in these settings use it as an on-demand tool, i.e. used only when there are signs or symptoms suggesting hemodynamic or respiratory change. US is also more prevalently used during the initial or unstable stage of care and less so when the patient is more stable. The authors goal was to see if routine use of US during morning rounds on all patients would improve patient outcomes.
Questions
Does routine use of POCUS during morning rounds improve patient outcomes?
Population
Single University Hospital in Hangzhou China (Sir Run Run Shaw)
Inclusion:
- Patients with sepsis (defined as infection + signs of organ dysfunction)
Exclusion:
- Pregnancy
- Advanced stage of malignancy
- Younger than 18 years old
- Missing values on mortality outcome
- DNR
Design
Prospective case control study
Three medical teams in the ICU (Attending, two fellows, and three residents).
Two served as control and used POCUS as needed and third was intervention group that did daily US rounds.
They used a checklist for their scans developed under the international guideline of critical care ultrasonography
Treatment changes were recorded and reviewed.
Primary outcome was hospital mortality. Secondary outcomes were ICU length of stay, duration of mechanical ventilation, duration of vasopressors.
Multivariable logistic regression taking into account APACHE II score, age, mechanical ventilation, vasopressors, infection site, and fluid balance through day 3.
Who did the ultrasounds?
Providers in the intervention group.
Had a one week course endorsed by WINFOCUS, attendings, fellows, residents
The Scan
They used all transducers, different ones for the various scans below


5 Minutes Sono – Cardiac Function
5 Minute Sono – Volume Responsiveness

The POCUS Atlas – Echo Pathology
The POCUS Atlas – Pulmonary Pathology
Results
The Patients
129 patients met criteria and were enrolled
No significant differences in patient population between Intervention (n=41) and Control (n=88)
Primary Outcomes
Mortality
No statistically significant difference
Mortality trended lower in the intervention group (0.27 vs 0.43, p=0.113)
Mechanical Ventilation
Shorter duration of mechanical ventilation in intervention (POCUS) group
5.7 ±1 vs 4.5 ±1.2, p= 0.034
Vasopressors and Length of Stay
No significant different in vasopressor days
No significant difference in LOS in ICU (7.2 control Vs 6.9 intervention, p = 0.055)
Other Findings
Fluid Balance
Sig difference in fluid balance on day 3
Control 48 ml vs Intervention -143 ml)
Unclear because also stated the difference was “a few hundred milliliters” in discussion
POCUS used more in intervention group
- 283 times in Intervention group
- 53 times in control
Modified diagnosis in 8 patients (19.5%) confirmed suspicion in 21 (51.2%).
Changed fluid management 81 times (28.6%), vasoactive agents 53 times (18.7%), added diuretics 71 times (25.1%)
In logistic regression model POCUS significantly reduced the likelihood of prolonged ICU stay (OR 0.39). There was also a significant difference in fluid balance.
Mechanical ventilation and Vasopressors were associated with mortality and ICU stay.
Limitations
Outside of US, single center – may have other factors affecting care. This limits external validity.
Not randomized or blinded. Did the intervention group try harder to wean MV or pressors? The differences between groups seen in this data could be due to practice variability between the intervention attending vs the control attendings. They did try to mitigate this through protocols.
Discussion
Use of routine POCUS did not show a mortality benefit as intended in the study but did show a shortened duration of mechanical and vasopressor use. Why? This could be because small sample size or that it may not matter. Only larger, more well-designed studies will tell.
Fluid balance was significantly less in intervention group on days 2 and 3. Could this be the cause of the difference in length of stay or vasopressor use? On the other hand, the balance was different by a few hundred milliliters – unlikely of clinical significance. Intuitively, having a POCUS protocol could be a few benefits to the patients – 1) early diagnosis and treatment of causes or sepsis or complications 2) Fluid management. Perhaps there is a certain patient population that would benefit most from this protocol – those with an unclear diagnosis or unclear fluid status. Perhaps isolating these patients would show a more robust benefit.
Take Home Points
1. Protocolized daily US rounds in the ICU may lead to modest improvements in outcomes such as length of stay and duration of mechanical ventilation.
2. Larger studies are needed to confirm these results, determine if mortality benefit, and suggest the mechanism for these benefits.
Our score





