Author: Ashley Phipps, MD (EM Resident Physician, UTSW/Parkland Memorial Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (EM Resident Physician, SAUSHEC, USAF)
A 76 year-old male with past medical history of crack cocaine abuse, alcoholic liver cirrhosis, COPD, and panhypopituitarism s/p resection of a pituitary adenoma presents to the ED with altered mental status, vomiting, and diarrhea. Per the patient’s wife, he recently went on a 3-day crack cocaine binge and now for the past 2 days has been increasingly confused and unable to take anything by mouth including his medications. His wife denies any fevers, dyspnea, or hematemesis.
The patient’s vitals are pertinent for significant hypotension (60s/40s) after receiving a 1L NS bolus, tachycardia, and tachypnea. Physical exam reveals a confused elderly man able to answer some orientation questions, but giving inappropriate responses to questions and unable to follow commands. He has dry mucus membranes. Lungs are clear to auscultation bilaterally, heart sounds are normal, his abdomen is soft, non-tender, with no fluid wave, no lower extremity edema is present, and no gross melena or hematochezia is found. A chest x-ray is unremarkable. POC glucose reveals hypoglycemia and one amp of D50 is given with no improvement in mental status. Laboratory studies show a normal ABG, CBC, and chemistry except for K+ 2.8. A random cortisol level returns at 4 micrograms/dL.
The patient is admitted to the MICU for concerns of acute adrenal crisis and started on IV fluids and stress-dose steroids. Several hours after the first dose of steroids, the patient begins improving clinically and has complete resolution of symptoms and normalization of vitals by the next morning. The patient is discharged home the following day.
Background
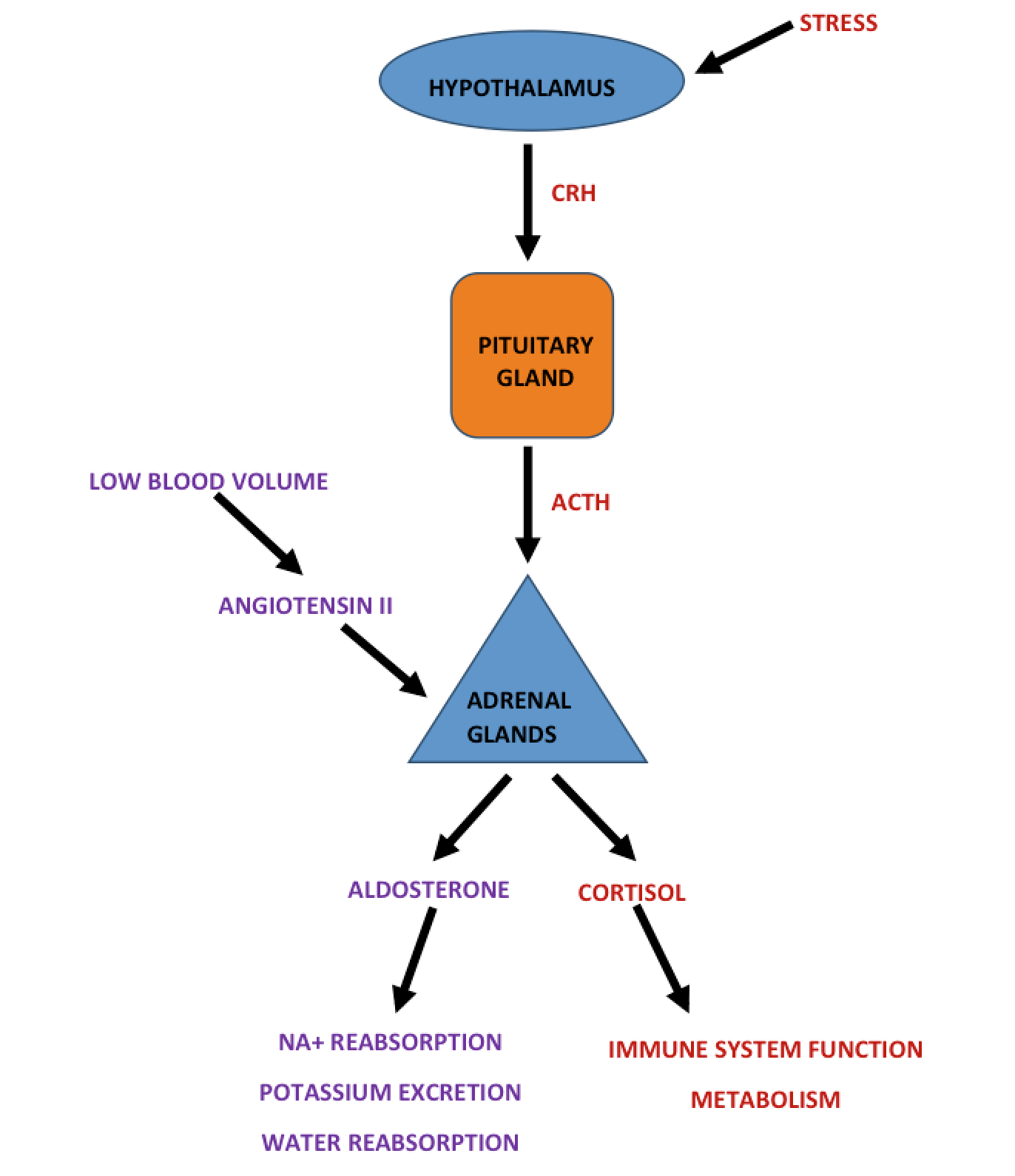
The adrenal glands are retroperitoneal organs important for producing mineralocorticoids, glucocorticoids, and androgens in the outer cortex and catecholamines in the inner medullary zone. One of the most important glucocorticoids is cortisol. Cortisol is released during times of stress to assist with immune function, vascular tone, and metabolism. Cortisol release is regulated by the hypothalamic-pituitary-adrenal axis; therefore, any disruption in this axis can result in adrenal insufficiency.
Adrenal insufficiency is estimated to affect 1-4 people per 100,000 in the US (1). The majority of these cases are due to primary adrenal insufficiency with >80% of the cases in the U.S. from Addison’s disease. Primary disease is due to direct disease of the adrenals. Other causes of primary adrenal insufficiency include trauma, drugs, infections, infiltrative disorders, and genetic disease. Patients with AIDS in particular have a 20% chance of developing adrenal insufficiency. Contrastingly, secondary adrenal insufficiency occurs with sudden termination of prolonged glucocorticoid therapy and pituitary disease including brain tumors, medication, necrosis or bleeding, infectious disease, and infiltrative disorders (2). Tertiary adrenal insufficiency due to hypothalamic disease is also possible.
Adrenal insufficiency can be difficult to diagnose as the symptoms are generally chronic, vague complaints. A recent retrospective study done in Poland showed that 44% of patients with adrenal insufficiency were only diagnosed after presenting in acute adrenal crisis (3). Although adrenal insufficiency can be insidious, when the body experiences a stressor the low cortisol levels are quickly depleted, and the body is unable to mount an appropriate response resulting in an adrenal crisis. The stress can be secondary to infection, surgery, trauma, and has even been shown to occur after strenuous exercise or emotional stress (6). Hahner et al. looked at 444 patients with chronic primary or secondary adrenal insufficiency to determine common precipitating factors for adrenal crisis. Fever or GI illness was the precipitating causes in 45% of adrenal crises. Additionally, in 6-12% of the patients no precipitant was ever identified (4).
Clinical Presentation
The hallmark clinical presentation of an adrenal crisis is severe hypotension refractory to IV fluids and vasopressors, occurring in >90% of cases (2). Other symptoms are vague and general including: dehydration, weakness, lethargy, altered mental status, delirium, flank pain, back pain, and chest pain. Gastrointestinal symptoms are fairly common including abdominal pain, anorexia, nausea, vomiting, and diarrhea with up to 22% of cases presenting with abdominal symptoms mimicking an acute abdomen (1,2). Clinical presentation will also differ based on the precipitating event and the complicating symptoms of that event.
Diagnostic Studies
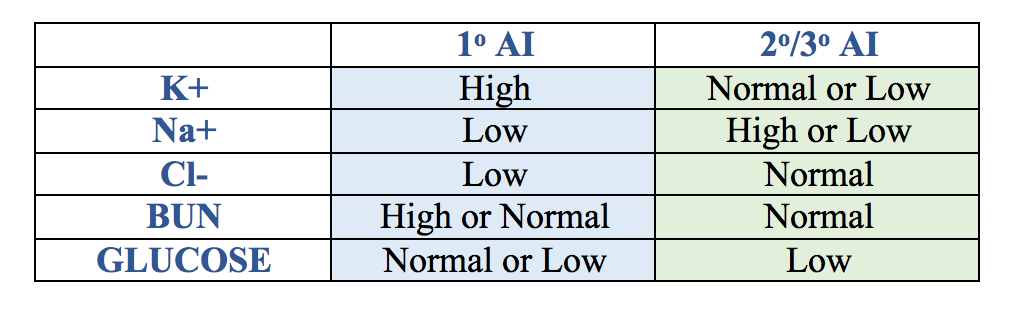
No diagnostic studies are required prior to starting treatment if adrenal crisis is suspected, as early treatment is associated with decreased morbidity and mortality. However, at a minimum basic labs should be obtained including blood counts and a chemistry panel. Primary electrolyte abnormalities vary based on whether the underlying adrenal insufficiency is primary or secondary.
Random cortisol levels are difficult to interpret in the acute seriously ill patient, but some studies have looked at this laboratory value. Generally, cortisol levels >34 micrograms/dL exclude the diagnosis of adrenal crisis and levels <15 micrograms/dL suggest the diagnosis. However, this is further complicated by the amount of corticosteroid-binding globulin, which varies in patients undergoing physiologic stress. This often makes free cortisol levels unreliable (5).
A rapid ACTH stimulation test can also be performed, though this is usually not an ED test. To do this, a baseline cortisol level is drawn followed by the administration of Cosyntropin 0.25 mg IV (synthetic ACTH) with repeat cortisol levels drawn at 30 mins and 1 hr post administration. The cortisol levels should rise at least 7 micrograms/dL and peak at >18 micrograms/dL to rule out adrenal insufficiency. Subsequently, ACTH levels can then be measured to determine if the insufficiency is due to a primary or secondary cause.
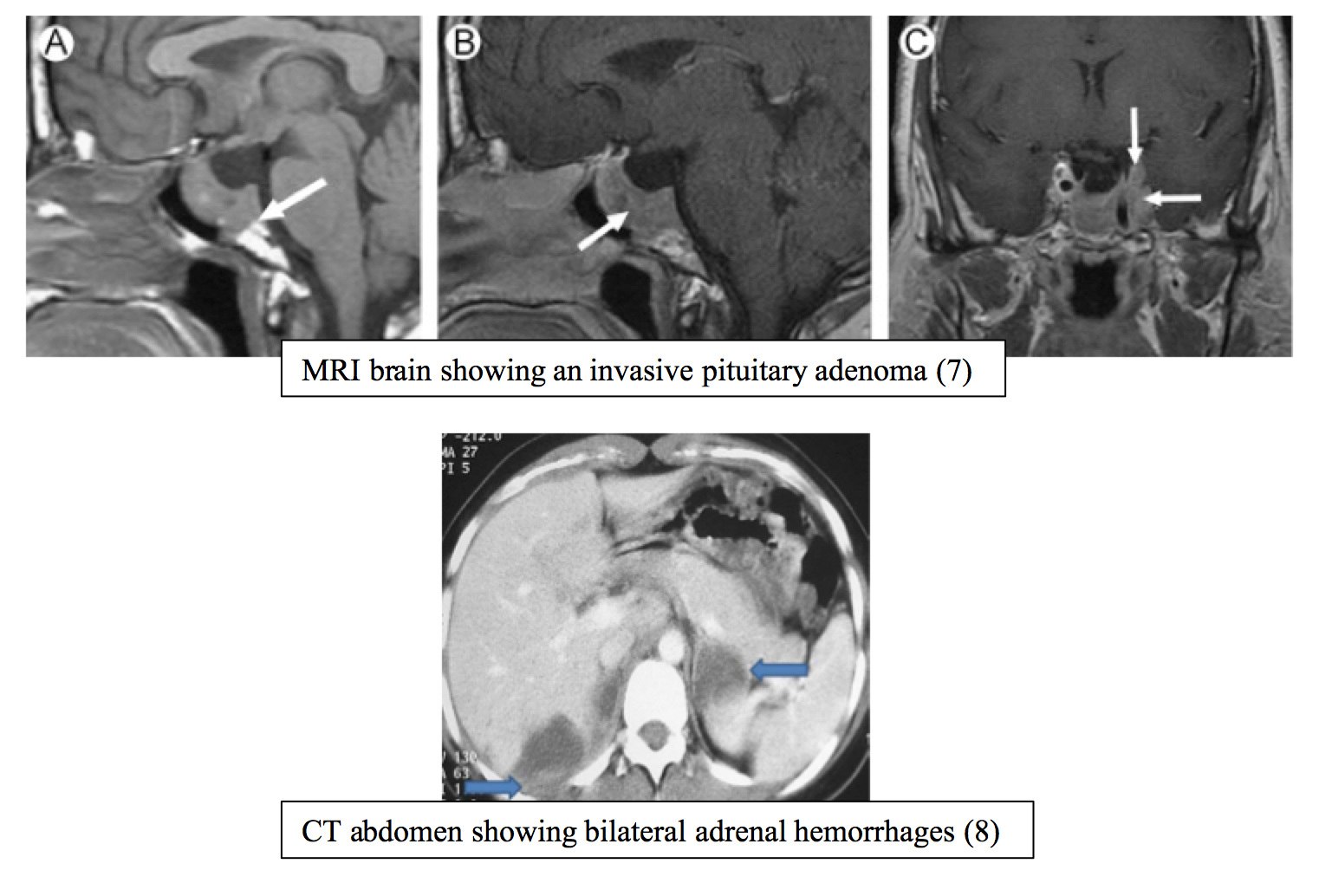
Imaging is generally not necessary for patients with known history of adrenal insufficiency and is often negative. However, if the diagnosis is still unclear a CT head or MRI brain may show destruction or tumor of the pituitary gland if the patient has secondary adrenal insufficiency or a CT abdomen may show adrenal calcifications, tumors, or hemorrhages if primary adrenal insufficiency is present (2).
Further studies should be performed as indicated to identify the precipitating event.
Management
As soon as adrenal crisis is suspected, steroids should be given. Hydrocortisone is the steroid of choice, as it has both glucocorticoid and mineralocorticoid effects. Patients 12 years and older should receive 100 mg IV initially and then 100 mg IV every 8 hours after that until the acute crisis resolves. For children ages 3-12 years old, dosing should be reduced to 50 mg IV and for infants <3 years old reduced further to 25 mg IV. Dexamethasone 4 mg IV is also an option and preferred by some physicians as it will interfere less with a rapid ACTH simulation test (1).
Fluid hydration in the form of IV fluid boluses should be given, with up to 2-3 L often required in the initial resuscitation stages to treat any concurrent dehydration. Afterwards, IV hydration with D5 NS can be beneficial, as it will help correct the hypoglycemia and hyponatremia often seen in these patients. Vasopressors can be started as needed, although these patients’ hypotension can be refractory to both fluids and vasopressors. Steroids are ultimately needed for vascular tone. The precipitating cause should be treated as indicated (1,2).
Most patients will need admission to the ICU for close monitoring and blood pressure management.
Summary
Adrenal crisis is a life-threatening emergency that needs to be recognized and treated quickly in the ED to prevent subsequent morbidity and mortality. Approximately half of patients will have no past medical history of adrenal insufficiency. The hallmark of the disease is hypotension refractory to IV fluids and vasopressors. Treat empirically with hydrocortisone and treat any precipitating causes.
References/Further Reading
- Tintinalli JE et al. Adrenal insufficiency and adrenal crisis. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 2011; 7.
- Tucci V, Sokari T. The clinical manifestations, diagnosis, and treatment of adrenal emergencies. Emerg Med Clin North Am. 2014; 32(2): 465-484. http://www.ncbi.nlm.nih.gov/pubmed/24766944
- Papierska L, Rabijewski M. Delay in diagnosis of adrenal insufficiency is a frequent cause of adrenal crisis. Int J Endocrinol. 2013. http://www.ncbi.nlm.nih.gov/pubmed/23864857
- Hahner S, Loeffler M, Bleicken B, Drechsler C, Milovanovic D, Fassnacht M, Ventz M, Quinkler M, Allolio B. Epidemiology of adrenal crisis in chronic adrenal insufficiency: the need for new prevention strategies. Eur J Endocrinol. 2010; 162(3): 597-602. http://www.ncbi.nlm.nih.gov/pubmed/?term=adrenal+crisis+in+chronic+adrenal+insufficiency+the+need+for+new
- Cooper M, Stewart P. Corticosteroid insufficiency in acutely ill patients. N Eng J Med. 2003; 348(8): 727-734. http://www.ncbi.nlm.nih.gov/pubmed/12594318
- Allolio B. Extensive expertise in endocrinology. Adrenal crisis. Eur J Endocrinol. 2015; 172(3): 115-124. http://www.ncbi.nlm.nih.gov/pubmed/25288693
- Vattoth S et al. Endocranial lesions. Seminars in Ultrasound, CT, and MRI. 2013; 34(5): 393-411. http://www.ncbi.nlm.nih.gov/pubmed/24216450
- Gupta P et al. Bilateral adrenal lesions. J Med Imaging and Radiation Oncology. 2012; 56: 636-645. http://www.ncbi.nlm.nih.gov/pubmed/23210583
- http://www.ncbi.nlm.nih.gov/pubmed/23823267





4 thoughts on “Adrenal Crisis in the ED”
Pingback: Endocrine Emergencies – rathemblog
Pingback: Asynchronous Learning: Endocrine, Metabolic, Nutritional - Bold City Emergency Medicine
Pingback: emDOCs.net – Emergency Medicine EducationMimics of Sepsis: What do ED Physicians Need to Know? - emDOCs.net - Emergency Medicine Education
Pingback: 19-year-old Woman with Intermittent Weakness - The Western Journal of Emergency Medicine