Authors: Daniel Reschke, MD (EM Resident Physician, San Antonio, TX) and Zachary Sletten, MD (EM Attending Physician, San Antonio, TX) // Edited by: Alex Koyfman, MD (@EMHighAK) and Brit Long, MD (@long_brit)
Case
A 50-year-old female with a history of end stage renal disease (ESRD) on dialysis and hypertension presents to your ED with chief complaint of a painful rash. She explains that for the past week she developed painful nodules on her abdomen, which now seem to be appearing on both breasts. She has some nausea but denies any other symptoms. She also notes a history of prior DVT/PE and lupus anticoagulant syndrome, for which she is taking warfarin.
Vital Signs: BP 98/40, HR 100, RR 18, T 36.7, SpO2 99% RA. Physical exam reveals an obese female in moderate distress. Skin findings are significant for multiple eschars with ulcerations located on bilateral breasts, pannus, and buttocks. The area surrounding the eschars is firm and tender. A few of the wounds are weeping purulent fluid.
What is your differential? What medical condition should clue you into the likely diagnosis? What is an appropriate disposition?
 Background
Background
There are a few critical skin conditions to consider in the emergency department such as necrotizing fasciitis, TENS, Steven Johnsons, DRESS, and others, but another should be added to your list. Calciphylaxis is a rare, poorly understood, life threatening disease where calcification of microvessels leads to painful skin lesions and necrotic ulcers. It most commonly affects patients with ESRD and patients on dialysis. [1-3] Although the exact pathogenesis has not been clearly defined, it is thought that calcified, narrowed microvessels lead to chronic ischemia until finally an ischemic event occurs. [1-2] Often the triggering event is never identified, however skin trauma has a clear association. [4] Calciphylaxis has an incidence of 6 cases per 10,000 chronic hemodialysis patients, is still under recognized, and unfortunately is becoming increasingly prevalent. [5] Once identified, it carries an ominous 6 month mortality of 30-60%. [4,6] Especially in its early stages, a high clinical suspicion is required to make the diagnosis. Patients experiencing calciphylaxis should be admitted, sometimes requiring ICU level care or even consideration of a burn center transfer.
History and Exam
Classic risk factors for calciphylaxis include history of ESRD, female sex, obesity, hyperparathyroid, and use of certain medications (especially warfarin, calcium, and vitamin D). Among patients with ESRD who are taking warfarin concomitantly, the risk increases by 3 to 13-fold. [1] Symptoms appear approximately 30 months after the initiation of hemodialysis. [4]
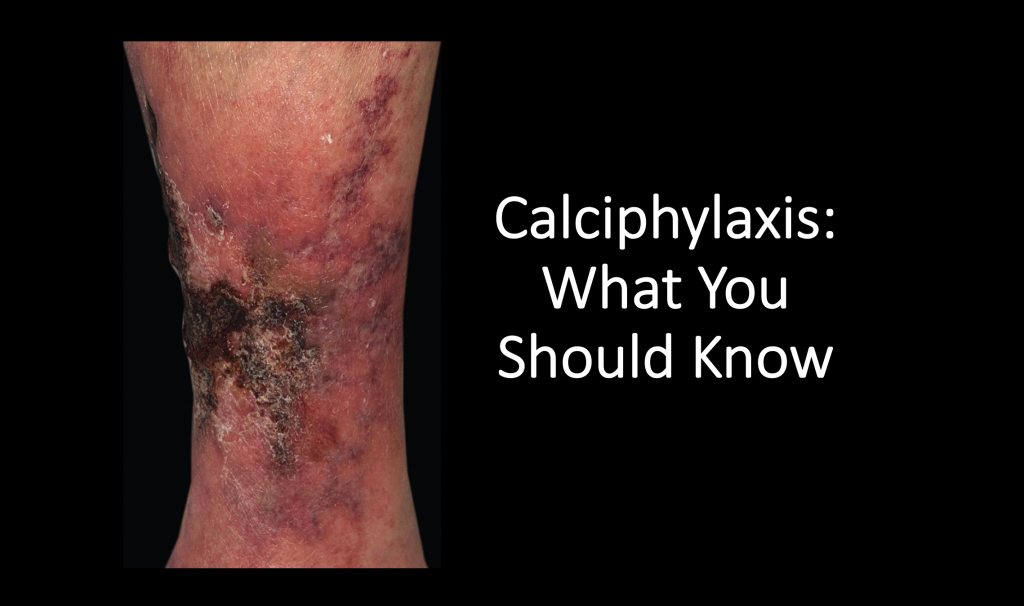
Patients report the development of painful skin lesions with appearance ranging from reticular erythema and nodules to necrotic ulcers with eschars. Lesions develop over several days to weeks and are typically located in areas of adipose deposition such as the breasts, abdomen, buttocks, and thighs.[7] These lesions are often multiple and bilateral, and in patients with ESRD, they tend to be more centrally located compared to patients without ESRD. [2,8]
Differential Diagnosis
A variety of other conditions can present similarly, including necrotizing fasciitis, cellulitis, warfarin induced skin necrosis (WISN), DIC, vasculitis, venous stasis ulcer, and cutaneous anthrax. It may be difficult to differentiate calciphylaxis from these other disease processes. The classic history of an ESRD patient on warfarin with painful ulcers/eschars distributed to adipose tissue will point to calciphylaxis. Necrotizing fasciitis classically presents acutely, involves the extremities, and is associated with recent trauma or surgery. WISN generally presents within 10 days of initiating warfarin therapy, DIC will have abnormal coagulation labs, and stasis ulcers are generally irregular and located near the distal tibia. [2]
Diagnostics
Diagnosis is largely clinical and based on skin findings with classic risk factors. Lab evaluation is aimed at ruling out other disease processes and should include baseline kidney function (Cr, BUN), infectious work-up (CBC, blood cultures), and coagulation studies (PT, PTT, INR, fibrinogen). Classically calcium, PTH, and phosphorus are abnormal; however, more recent reports indicate these values are non-specificPlain films may show microvascular calcifications, but this is neither sensitive nor specific.[1] Use of CT, MRI, US has not been well described in the available literature. Skin biopsy is the gold standard for confirmation in atypical presentations
Management
As it may be difficult to differentiate this condition from other life-threatening rashes, resuscitation while the patient is in the ED may be needed based on patient appearance and hemodynamic status, with a low threshold to initiate antibiotics given the propensity for the necrotic lesions to lead to sepsis. Patients will require analgesia due to significant pain. These patients are high risk for other clinical conditions given calcification of other organs to include coronary arteries. There are no approved therapies, however novel treatments are being investigated and may be initiated once admitted under the care of specialists. A potential treatment that may be considered is hyperbaric oxygen therapy and some medications, to include sodium thiosulfate, have shown promise. [1] Avoid unnecessary skin trauma (i.e. multiple IV attempts), which can precipitate new lesions.
Disposition
Due to the high mortality and wound care needs these patients need admission, likely to an ICU, for interdisciplinary care (i.e. dermatology, nephrology, wound care etc.). The most common cause of death among patients with calciphylaxis is sepsis. [8-9] In one study, sepsis contributed to the cause of death in 41% of cases. [10] Patients may recover from this disease, but it carries a very poor prognosis as stated above. The available literature does not have data on recurrence rates.
Case Resolution
The patient was admitted to the burn ICU, where she had a full thickness biopsy of the lesions that was consistent with calciphylaxis. Treatment was attempted with cinacalcet and sodium thiosulfate, but ultimately the patient developed gram negative bacteremia and died from septic shock.
References/Further Reading
- Nigwekar, Sagar U., et al. “Calciphylaxis.” New England Journal of Medicine, vol. 378, no. 18, 2018, pp. 1704–1714., doi:10.1056/nejmra1505292.
- Jeong, Haneol S., and Arturo R. Dominguez. “Calciphylaxis: Controversies in Pathogenesis, Diagnosis and Treatment.” The American Journal of the Medical Sciences351.2 (2016): 217-27. Print.
- Brandenburg, Vincent M., et al. “Calcific Uraemic Arteriolopathy (Calciphylaxis): Data from a Large Nationwide Registry.” Nephrology Dialysis Transplantation, 2016, doi:10.1093/ndt/gfv438.
- Nigwekar, Sagar U., et al. “A Nationally Representative Study of Calcific Uremic Arteriolopathy Risk Factors.” Journal of the American Society of Nephrology, vol. 27, no. 11, 2016, pp. 3421–3429.
- Nigwekar, Sagar U., et al. “Quantifying a Rare Disease in Administrative Data: The Example of Calciphylaxis.” Journal of General Internal Medicine, vol. 29, no. S3, 2014, pp. 724–731.
- McCarthy, James T, et al. “Survival, Risk Factors, and Effect of Treatment in 101 Patients With Calciphylaxis.” Mayo Clinic Proceedings, vol. 91, no. 10, Oct. 2016, pp. 1384–1394.
- Ghosh, Toshi, Daniel S. Winchester, Mark D.P. Davis, Rokea El-Azhary, and Nneka I. Comfere. “Early Clinical Presentations and Progression of Calciphylaxis.” International Journal of Dermatology56.8 (2017): 856-61.
- Nigwekar, Sagar U., et al. “Calciphylaxis: Risk Factors, Diagnosis, and Treatment.” American Journal of Kidney Diseases, vol. 66, no. 1, 2015, pp. 133–146.
- Fine, Adrian, and James Zacharias. “Calciphylaxis Is Usually Non-Ulcerating: Risk Factors, Outcome and Therapy.” Kidney International, vol. 61, no. 6, 2002, pp. 2210–2217.
- Weenig, Roger H, et al. “Calciphylaxis: Natural History, Risk Factor Analysis, and Outcome.” Journal of American Academic Dermatology, Apr. 2007, pp. 569–579.
Image: Scola, N., and A. Kreuter. “Calciphylaxis: A Severe Complication of Renal Disease.” Canadian Medical Association Journal183.16 (2011): 1882. Print.





2 thoughts on “Calciphylaxis: An Ominous Skin Condition You Should Know About”
Very interesting case and something that could be easily overlooked. I will definitely keep this on my radar. Great job.
Pingback: Länkar v13-14 | Internmedicin