Today on the emDOCs cast with Brit Long, MD (@long_brit), we discuss the ED evaluation of suspected diverticulitis.
Episode 88: ED Evaluation of Diverticulitis
Background:
- Diverticulosis is common: it affects 30% of those age 60 years and up to 80% of those over 80 years.
- 5-10% of patients with diverticulosis will experience diverticulitis (inflammation of diverticula).
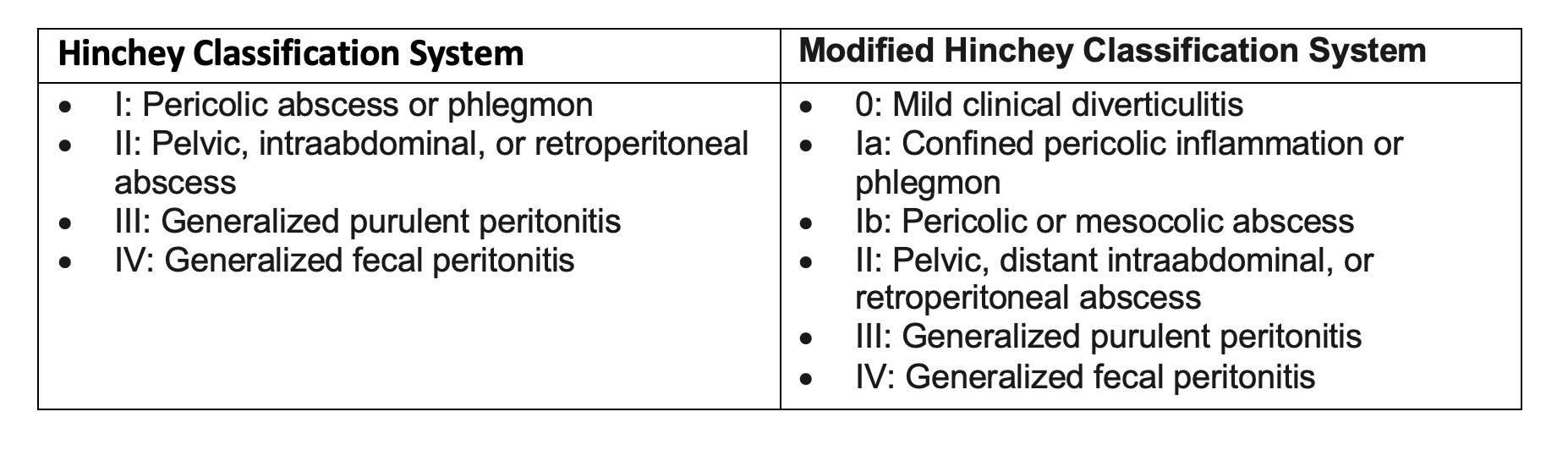
- Diverticulitis is divided into uncomplicated and complicated (abscess, fistula, perforation).
- Categorization is primarily based on imaging (e.g., Hinchey).
Assessment:
- Several factors are associated with diverticulitis.
- Clinical assessment is accurate in 25-75% of patients with diverticulitis.
- The most common symptom is LLQ pain for left sided diverticulitis. A history of LLQ pain has a +LR of 3.3 and a -LR of 0.5. Tenderness in the LLQ has a +LR of 10.4, with a -LR of 0.7.
- 50% will have constipation, 25-35% will have diarrhea.
- Absence of vomiting has a -LR of 0.2, but a +LR of only 1.4.
- Up to 15% can have urinary symptoms like dysuria due to bladder irritation.
- Fever may be present.
- Severe pain, guarding, rigidity suggest complication.
Laboratory analysis:
- WBC is not sensitive or specific
- CRP and neutrophil to lymphocyte ratio may assist in determining the risk of complication.
- CRP > 50 mg/L associated with diverticulitis; levels > 175-200 mg/dL are associated with complicated diverticulitis.
- Do not use labs to exclude the diagnosis.
Prediction Rules/Risk Scores:
- Several tools are available that combine history, exam, labs
- One study evaluated three predictors to evaluate for complicated diverticulitis: absence of vomiting, a C-reactive protein level greater than 5 mg/dL (50 mg/L), and tenderness limited to the left lower quadrant (Lameris).
- The presence of all three demonstrated a sensitivity of 36% (95% CI, 26% to 47%), specificity of 98% (95% CI, 89% to 100%), +LR of 18, and -LR of 0.65 (Lameris) for diagnosis of complicated diverticulitis.
- Validation found sensitivity of 37% (95% CI 29% to 46%) and specificity 93% (95% CI 88% to 96%), +LR of 5.29, and -LR of 0.68 (Kiewiet).
- A 2018 risk score incorporates the presence of abdominal guarding, WBC, and CRP. CRP < 10 mg/dL, WBC 15,000 or lower, and no abdominal guarding demonstrated a 4.2% rate of complicated diverticulitis. Those with abdominal guarding, WBC over 20,000, and CRP over 25 mg/dL demonstrated a risk of complicated diverticulitis of over 85% (Bolkenstein 2018).
- Systematic review found increasing age, diffuse rather than localized abdominal pain, guarding or pain with rebound, initial episode of diverticulitis, steroid use, fever, constipation and vomiting, elevated CRP, and elevated WBC count were associated with greater risk of complication such as abscess or perforation (Bolkenstein 2017).
Imaging:
- Plain radiography not helpful unless using it to evaluate for perforation
- Computed tomography (CT) of the abdomen and pelvis with IV contrast is the primary imaging modality utilized for diagnosis of diverticulitis and complication
- Several major societies have guidelines on imaging.
- World Society of Emergency Surgery guidelines (2020)
- “What is the best way to make a diagnosis of ALCD? In patients with suspected ALCD, we suggest a complete assessment of the patients using clinical history, signs, laboratorial inflammation markers, and radiological findings (weak recommendation based on very low-quality evidence, 2D).”
- “In patients with suspected, ALCD we suggest against diagnosis based only on clinical examination (weak recommendation based on very low-quality evidence, 2D).”
- The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines (2020)
- “The initial evaluation of a patient with suspected acute diverticulitis should include a problem-specific history and physical examination and appropriate laboratory evaluation. Grade of Recommendation: Strong recommendation based on low-quality evidence, 1C.”
- “CT scan of the abdomen and pelvis is the most appropriate initial imaging modality in the assessment of suspected diverticulitis. Grade of Recommendation: Strong recommendation based on moderate-quality evidence, 1B.”
- “Computed tomography imaging has become a standard tool to diagnose diverticulitis, assess disease severity, and help devise a treatment plan.”
- American Gastroenterological Association (2021)
- Best Practice Advice 1: Computed tomography should be considered to confirm the diagnosis of diverticulitis in patients without a prior imaging-confirmed diagnosis and to evaluate for potential complications in patients with severe presentations. Imaging should also be considered in those who fail to improve with therapy, are immunocompromised, or who have multiple recurrences and are contemplating prophylactic surgery in order to confirm the diagnosis and location(s) of disease.
- American College of Radiology ACR Appropriateness Criteria (2023)
- Left lower quadrant pain. Initial imaging. This variant applies if there is nonspecific pain in the left lower quadrant with a broad differential diagnosis including gastrointestinal, gynecologic, urologic, and body wall pathology. CT is the most useful examination for left lower quadrant pain. It is accurate and guides appropriate management, regardless of patient sex or patient body habitus. CT is sensitive for small quantities of extraluminal intraperitoneal or retroperitoneal air
- Left lower quadrant pain. Suspected diverticulitis. Initial imaging. Imaging may not be required in certain patients with typical symptoms of diverticulitis, a prior history of diverticulitis with similar symptoms, and no evidence of complication(s). However, there has been a trend toward greater use of imaging to confirm the diagnosis of diverticulitis, evaluate the extent of disease, and detect complications before deciding on appropriate treatment. This is due to complications such as perforation, abscess, fistula, or obstruction that may require surgery or interventional radiology management. Additionally, misdiagnosis based on clinical assessment alone is common.
- Left lower quadrant pain. Suspected complication(s) of diverticulitis. Initial imaging. CT is the most useful examination for patients with suspected complications of colonic diverticulitis because of its reproducibility, superior diagnostic accuracy (98%)m accuracy for alternative diagnoses with a similar presentation, risk-stratification of patients for operative versus nonoperative treatment, and inpatient versus outpatient triage.
- American College of Physicians (2022)
- Recommendation 1: ACP suggests that clinicians use abdominal CT imaging when there is diagnostic uncertainty in a patient with suspected acute left-sided colonic diverticulitis (conditional recommendation; low-certainty evidence).
- A detailed history, physical examination, and laboratory findings are the first steps in diagnosing acute colonic diverticulitis in most patients with abdominal pain or tenderness primarily in the left lower quadrant. In patients for whom diagnostic uncertainty remains, abdominal CT imaging can be used to complement the history, examination, and laboratory findings to establish the diagnosis of diverticulitis. Diagnostic uncertainty will vary on the basis of an individual clinician’s experience and may particularly occur for patients without a history of diverticulitis or those with signs and symptoms pointing toward an alternative diagnosis (such as cancer, gynecologic or renal causes of acute abdomen, or inflammatory bowel disease).
- Moderate-certainty evidence showed that CT imaging is associated with very high sensitivity and specificity to make an accurate diagnosis of diverticulitis. However, no included studies compared patient health outcomes between CT-guided care and care without the use of routine CT for suspected diverticulitis.
- Clinicians should err on the side of imaging in patients with predictors of progression to complicated diverticulitis. These risk factors are immunosuppression, recent or current antibiotic use, signs of sepsis, symptoms > 5 days, unstable comorbidity, vomiting, CRP > 14 mg/dL or 140 mg/L, or if there are signs of perforation, bleeding, obstruction, or abscess.
- American Family Physicians
- Imaging should be considered if the diagnosis is uncertain or there is concern for complicated diverticulitis.
- Diverticulitis is considered complicated in patients with abnormal vital signs, signs of perforation with or without abscess, fistula or obstruction, or the inability to maintain oral intake.
- Patients with complicated acute diverticulitis should be admitted to the hospital. Computed tomography with intravenous contrast should be obtained for patients with vital sign abnormalities or if there is a concern for abscess, perforation, or fistula.
- If imaging is performed, computed tomography with contrast is the diagnostic test of choice because of its availability and high sensitivity (94%) and specificity (99%).


- US for Diverticulitis
- First line imaging modality in some regions.
- It can be over 90% accurate.
- Diagnose diverticulitis with 1. Short-segment colonic wall thickening (>5 mm) 2. Inflamed diverticulum in the thickened area (hypoechoic and surrounded by hyperechoic fat) 3. Noncompressible hyperechoic pericolic tissue. I just don’t think this is ready for primetime, especially in the U.S.
- Limitations: operator dependent, may be inconclusive, is not reliable for diagnosing complications.
- At this time, likely not ready for routine use.
References:
- Wilkins T, Embry K, George R. Diagnosis and management of acute diverticulitis. Am Fam Physician. 2013 May 1;87(9):612-20.
- Peery AF. Management of colonic diverticulitis. BMJ. 2021 Mar 24;372:n72.
- Strate LL, Peery AF. Tips for the Medical Management of Diverticulitis. Am J Gastroenterol. 2023 Apr 1;118(4):585-589.
- Ferzoco LB, Raptopoulos V, Silen W. Acute diverticulitis. N Engl J Med. 1998 May 21;338(21):1521-6.
- Sartelli M, Weber DG, Kluger Y, et al. 2020 update of the WSES guidelines for the management of acute colonic diverticulitis in the emergency setting. World J Emerg Surg. 2020 May 7;15(1):32.
- Hall J, Hardiman K, Lee S, et al; Prepared on behalf of the Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Treatment of Left-Sided Colonic Diverticulitis. Dis Colon Rectum. 2020 Jun;63(6):728-747.
- Peery AF, Shaukat A, Strate LL. AGA Clinical Practice Update on Medical Management of Colonic Diverticulitis: Expert Review. Gastroenterology. 2021 Feb;160(3):906-911.e1.
- American College of Radiology ACR Appropriateness Criteria Left Lower Quadrant Pain. https://acsearch.acr.org/docs/69356/Narrative?_gl=1*17a9ia5*_ga*NzYxMTc5NDA4LjE2ODI5MjI1Mzc.*_ga_K9XZBF7MXP*MTY4MjkyMjUzNi4xLjEuMTY4MjkyMjUzNi4wLjAuMA..&_ga=2.79820816.681757303.1682922537-761179408.1682922537
- Qaseem A, Etxeandia-Ikobaltzeta I, Lin JS, et al; Clinical Guidelines Committee of the American College of Physicians. Diagnosis and Management of Acute Left-Sided Colonic Diverticulitis: A Clinical Guideline From the American College of Physicians. Ann Intern Med. 2022 Mar;175(3):399-415. doi: 10.7326/M21-2710. Epub 2022 Jan 18. Erratum in: Ann Intern Med. 2023 Apr;176(4):584.
- Toorenvliet BR, Bakker RF, Breslau PJ, et al. Colonic diverticulitis: a prospective analysis of diagnostic accuracy and clinical decision-making. Colorectal Dis. 2010 Mar;12(3):179-86.
- Jamal Talabani A, Endreseth BH, et al. Clinical diagnostic accuracy of acute colonic diverticulitis in patients admitted with acute abdominal pain, a receiver operating characteristic curve analysis. Int J Colorectal Dis. 2017 Jan;32(1):41-47.
- Mäkelä JT, Klintrup K, Takala H, Rautio T. The role of C-reactive protein in prediction of the severity of acute diverticulitis in an emergency unit. Scand J Gastroenterol. 2015;50(5):536-541.
- Tan JP, Barazanchi AW, Singh PP, Hill AG, Maccormick AD. Predictors of acute diverticulitis severity: A systematic review. Int J Surg. 2016;26:43-52.
- van de Wall BJ, Draaisma WA, van der Kaaij RT, et al. The value of inflammation markers and body temperature in acute diverticulitis. Colorectal Dis. 2013 May;15(5):621-6.
- Reynolds IS, Heaney RM, Khan W, et al. The Utility of Neutrophil to Lymphocyte Ratio as a Predictor of Intervention in Acute Diverticulitis. Dig Surg. 2017;34(3):227-232
- Laméris W, van Randen A, van Gulik TM, et al. A clinical decision rule to establish the diagnosis of acute diverticulitis at the emergency department. Dis Colon Rectum. 2010 Jun;53(6):896-904.
- Kiewiet JJ, Andeweg CS, Laurell H, et al. External validation of two tools for the clinical diagnosis of acute diverticulitis without imaging. Dig Liver Dis. 2014 Feb;46(2):119-24.
- Balk EM, Adam GP, Cao W, et al. Management of Colonic Diverticulitis [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2020 Oct. (Comparative Effectiveness Review, No. 233.)Available from: https://www.ncbi.nlm.nih.gov/books/NBK563756/
- Bolkenstein HE, van de Wall BJM, Consten ECJ, et al. Risk factors for complicated diverticulitis: systematic review and meta-analysis. Int J Colorectal Dis. 2017 Oct;32(10):1375-1383.
- Kechagias A, Rautio T, Kechagias G, et al. The role of C-reactive protein in the prediction of the clinical severity of acute diverticulitis. Am Surg. 2014 Apr;80(4):391-5.
- Kechagias A, Sofianidis A, Zografos G, et al. Index C-reactive protein predicts increased severity in acute sigmoid diverticulitis. Ther Clin Risk Manag. 2018 Oct 2;14:1847-1853.
- Bolkenstein HE, van de Wall BJ, Consten EC, et al. Development and validation of a diagnostic prediction model distinguishing complicated from uncomplicated diverticulitis. Scand J Gastroenterol. 2018 Oct-Nov;53(10-11):1291-1297.
- Sigurdardottir J, Chabok A, Wagner P, Nikberg M. Increased accuracy in diagnosing diverticulitis using predictive clinical factors. Ups J Med Sci. 2022 Dec 15;127.




