Author: Nachi Gupta, MD (EM Resident Physician, Department of EM, Mt. Sinai Hospital) // Edited by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Introduction
- Peripheral vascular injury can be life-threatening or limb-threatening. Proper understanding of pathology and management is important in the ER.
- Vascular injuries can be internal and may not be obvious on presentation. Patients with blunt or penetrating trauma who remain hypotensive after a fluid bolus challenge may have internal hemorrhage.
- Incidence of penetrating and blunt trauma in the US has been rising.
- Blunt and penetrating causes of peripheral vascular injuries are about equal in the US.
- Low velocity gunshot wounds are the second leading cause of death in the 15- to 34-year-old age group in the US. Peripheral vascular injury has been reported to be present in up to 50% of these cases.
General Management of Peripheral Vascular Injury
- Management of vascular injury should always start with ABCs. Ensure that the patient has a patent airway and good ventilation before assessing circulatory issues.
- Active bleeding should be controlled by direct pressure.
- Blind clamping of vessels can lead to nerve damage. However, a clearly visible vessel can be clamped to preserve hemostasis.
- A tourniquet can be applied if direct pressure and clamping are not sufficient. Using a tourniquet for up to six hours is considered safe in most instances.
- Large bore IVs should be placed immediately and not in the injured limb. For large bleeds, a type and cross should be initiated, as transfusion may be required.
- Target systolic blood pressure in hypotensive resuscitation is 90. Hypotensive resuscitation (or permissive hypotension) should be considered in cases of arterial injury, in which a clot that is preventing hemorrhage could blow off from a higher pressure.
- During active hemorrhage, there has also been a recent trend towards permissive hypotension. Actively bleeding patients receive less fluid resuscitation until hemorrhage is controlled. This is a widely debated topic (see http://lifeinthefastlane.com/ccc/permissive-hypotension/ and http://www.emdocs.net/foamed-roadmap-permissive-hypotension/ for more discussion).
Major Vascular Injuries
- Major vascular injuries should be repaired within six hours to prevent long-term damage.
- If the patient is hemodynamically unstable open surgical repair should be considered, otherwise endovascular repair with stenting might be preferred.
- Antibiotic use is recommended prior to and briefly after surgery.
- Vascular repair in the setting of complex fracture repair has been a topic of debate. Historically, orthopedic surgery was conducted first to ensure length of vascular graft was known. This resulted in a higher rate of postoperative fasciotomy. Now, most centers prefer to do the vascular repair first.
- Nerve damage often accompanies peripheral vascular injury due to the proximity of structures in neurovascular bundles. Suspect primary nerve injury if symptoms occur immediately following the injury. If the symptoms are delayed, vascular cause of neuropathy such as nerve compression and compartment syndrome are more likely.
Hard versus Soft Findings of Vascular Injury
- Hard findings
- Absent distal pulses
- Pulsatile bleeding
- Audible bruit
- Palpable thrill
- Expanding or pulsatile hematoma
- Distal signs of ischemia such as pallor, cyanosis, decreased temperature
- Soft findings
- Palpable but diminished (sometimes grouped with hard)
- Isolated peripheral nerve injury
- History of hemorrhage in the field
- Unexplained hypotension
- Complex fracture
- Stable, non-pulsatile hematoma
- Proximity of injury to major vascular structures
Specific Injuries
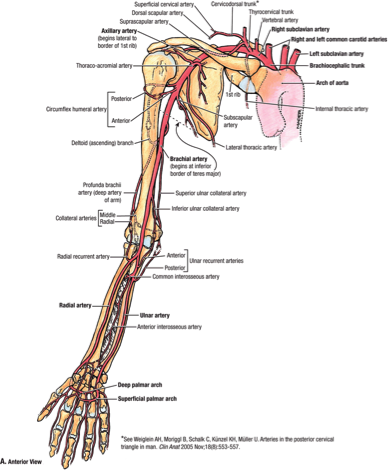
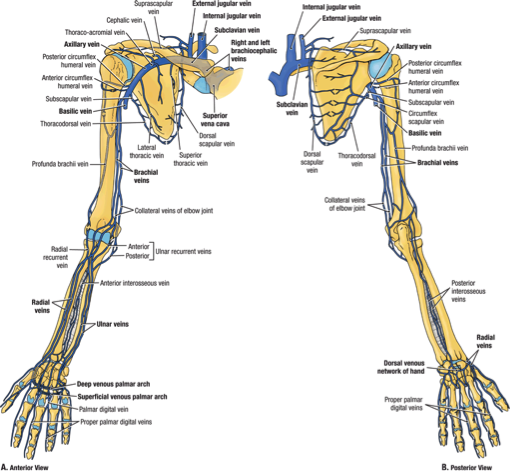
- Subclavian artery and vein injury
- Injury is uncommon, is usually due to penetrating trauma, and often manifests as hemorrhagic shock.
- About 60% of cases will also have a pneumothorax or hemothorax, and injury to mediastinal structures is common.
- Severe nerve injury can occur from blunt trauma damage to the brachial plexus
- In addition to CXR and physical exam, angiography can be very helpful in finding the exact location of the injury.
- Ultrasound is not very accurate in identifying the injury due to overlying pulmonary structures.
- Proximal/distal control of subclavian is very difficult and an incision along the clavicle is recommended, which may lead to a sternotomy.
- Blunt injuries have a higher mortality rate than penetrating because of higher rates of limb amputation or plexus injury.
- Blunt subclavian injury is often accompanied by clavicular dislocation or fracture.
- Subclavian vein injury is more lethal than artery due to the high risk of air embolus. Patients should be placed in Trendelenburg if vein injury is suspected.
- Axillary artery and vein
- Blunt trauma is often accompanied by shoulder dislocation and denervation due to plexus injury.
- There is a high risk of amputation if there is axillary vascular damage and plexus injury.
- Brachial artery
- This is the most common upper extremity vascular injury, and it is often seen with humeral shaft fracture, penetrating trauma, animal bites, and elbow dislocation.
- The radial pulse is often absent.
- These require immediate repair and have high success rate.
- Forearm arteries
- Forearm injuries need to be repaired if hard signs are present or both the radial and ulnar arteries are injured.
- Often injury to just radial or ulnar artery will require repair also to prevent intermittent claudication.
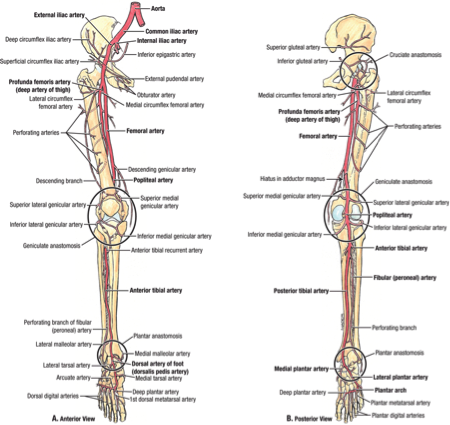
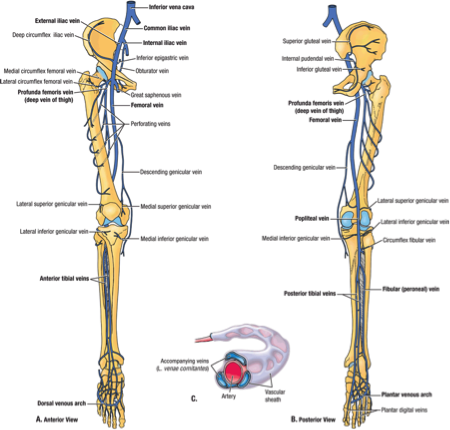
- Iliac artery and vein
- Often accompanied by injury to bowel, bladder, or bony pelvis.
- Massive bleeding can occur.
- Embolization using angiography may be necessary.
- Distal ischemic events can occur requiring future amputations.
- Femoral artery and vein
- Intertrochanteric hip fracture, hip dislocation, hip replacement, and penetrating trauma are common causes of injury to the femoral vessels.
- Ligation of the common femoral artery frequently results in distal amputation, so repair should always be attempted.
- Popliteal artery and vein
- Posterior knee dislocation is the most common cause of popliteal artery injury. It is possible with anterior knee dislocation also, though less common.
- Displaced fractures of the knee can also result in popliteal artery injury.
- Hemarthrosis may be absent if the joint capsule is torn as blood may flow into the leg.
- There is no consensus on the best diagnostic test for popliteal arterial injury in the setting of a concerning history. Options include:
- Arteriography for every case of knee dislocation.
- Rely completely on physical exam and non-invasive test(s) such as Ankle-Brachial Index and color flow Doppler.
- Arteriography or CTA scan only for cases that are inconclusive by non-invasive testing and physical exam.
- Diagnostic options are institution-specific, though the last option above is very popular.
- High-energy trauma such as MVA and penetrating trauma are more likely to cause arterial injury than low-energy sports-related trauma or blunt trauma.
- Popliteal injuries have a risk of distal amputations.
- Lower leg arteries
- Lower leg arteries often do not need repair, but have a high risk for compartment syndrome and require close monitoring.
- Lower leg arteries often do not need repair, but have a high risk for compartment syndrome and require close monitoring.


Final Remarks
- Peripheral vascular injury can be life- or limb-threatening. Treatment will vary depending on which specific vessel is injured.
- Be cognizant of hypotension that is not responsive to fluid bolus in a patient that has had blunt or penetrating trauma, as the patient may be bleeding internally.
- If following a hypotensive resuscitation protocol, monitor the systolic blood pressure closely to remain in a narrow therapeutic window. Avoid cycling between high systolic and low systolic pressures.
- Plan for repair of major vascular injuries within six hours and start antibiotics prior to surgery.
References
- Akuthota, V., & Herring, S. (2009). Nerve and vascular injuries in sports medicine. New York: Springer.
- Capone, A. C., Safar, P., Stezoski, W., Tisherman, S., & Peitzman, A. B. (1995). Improved outcome with fluid restriction in treatment of uncontrolled hemorrhagic shock. Journal of the American College of Surgeons, 180(1), 49-56.
- Holmes, J. F., Sakles, J. C., Lewis, G., & Wisner, D. H. (2002). Effects of delaying fluid resuscitation on an injury to the systemic arterial vasculature. Academic emergency medicine, 9(4), 267-274.
- Mattox, K. (2013). Trauma (7th ed.). New York: McGraw-Hill Medical.
- Patterson, B. O., Holt, P. J., Cleanthis, M., Tai, N., Carrell, T., & Loosemore, T. M. (2012). Imaging vascular trauma. British Journal of Surgery, 99(4), 494-505.
- Peng, P. D., Spain, D. A., Tataria, M., Hellinger, J. C., Rubin, G. D., & Brundage, S. I. (2008). CT angiography effectively evaluates extremity vascular trauma. The American Surgeon, 74(2), 103-107.
- Rosen, P., & Marx, J. (2014). Rosen’s emergency medicine: Concepts and clinical practice. (8th ed.). Philadelphia: Elsevier Saunders.
- Tintinalli, J. (2012). Tintinalli’s emergency medicine manual (7th ed.). New York: McGraw-Hill Medical.
- Wahlberg, E., Olofsson, P., & Goldstone, J. (2007). Emergency vascular surgery: A practical guide. Springer.
Images
- Agur, A., & Dalley, A. (2013). Grant’s atlas of anatomy (13th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.






1 thought on “Peripheral Vascular Injury Management”
Pingback: Nov 2017 Asynchronous Learning – Lakeland Health EM Blog