Authors: Kyle Barbour, MD (EM Resident Physician, University of Rochester, Rochester, NY) and Paolo Grenga, MD (EM Attending Physician, University of Rochester, Rochester, NY) // Reviewed by: Summer Chavez, DO, MPH, MPM (Health Policy Fellow, Georgetown University/Medstar); Alex Koyfman, MD (@EMHighAK); and Brit Long, MD (@long_brit)
Cases
A 27-year-old male rugby union player presents from the rugby pitch with pain and swelling around his right manubrium. Immediately prior to arrival, he was tackled and then buried under other players, one of whom landed on his lateral right shoulder. He felt immediate, intense pain in his central chest. He is mildly tachypneic to 22 breaths/minute and is hypoxic with an initial oxygen saturation of 89% on room air. It improves to 94% with supplemental oxygen by face mask. He is in exquisite pain and is exceptionally tender to his right manubrium. His right radial pulse is diminished. Any movement of the right shoulder worsens his pain. His initial 2-view chest x-ray shows a small right pneumothorax and 3-view shoulder x-rays are unremarkable.
A 46-year-old female presents to the emergency department after a motor vehicle collision. She was restrained and driving through an intersection when she was struck on the driver’s side by a pickup truck at approximately 45mph. Airbags deployed. She was placed in a cervical collar by EMS and transported uneventfully. She complains of neck, upper back, chest, and left shoulder pain. She has paraspinal neck tenderness and a palpable, tender, hard swelling on her left manubrium that becomes more prominent with left arm abduction. CT scans of the head and cervical spine without contrast are unremarkable as are 2-view chest and 3-view left shoulder X-rays.
Introduction
The sternoclavicular joint (SCJ) is an exceptionally stable and rarely dislocated synovial saddle joint required for nearly all shoulder movements.1–6 It is the only articulation of the shoulder with the axial skeleton.7,8 Its strength comes almost entirely from its robust ligamentous attachments, as the manubrium articulates with little of the medial clavicle.9,10 Dislocation requires rupture of all these attachments.1,2 When dislocated, the medial end of the clavicle can migrate anteriorly or posteriorly, with anterior dislocation far more common.1,2 The epiphyseal plate of the medial clavicle is the last ossification center in the body to fuse, doing so as late as the 3rd decade of life.4,8,11,12 As such, it is easy to misdiagnose younger patients with a Salter I or II medial clavicle fracture-dislocation as a sternoclavicular dislocation.1,5,6 Unlike posterior SCJ dislocations, physeal fracture-dislocations are less likely to require surgery and have a better prognosis.2,4,9
Anterior dislocations comprise the large majority of SCJ dislocations, in part due to the sturdy posterior capsule, which prevents posterior dislocation.4,9 Posterior dislocations, while rare, can be life-threatening due to damage of underlying structures and is an orthopedic emergency.1,2 SCJ dislocations comprise fewer than 1% of all dislocations and 3% of all shoulder girdle injuries; many orthopedic surgeons will never see one.1,6,8 Approximately 70–95% of SCJ dislocations are anterior.13 Anterior dislocations are non-life-threatening and easier to manage.1,2 Less serious SCJ injuries include sprains and subluxations.1,2
Posterior SCJ dislocations can compromise any of the anterior mediastinal structures.1–3 Most importantly, posterior dislocation can cause pneumothorax, disruption of the subclavian vein or artery, tracheal injuries, esophageal injuries, or brachial plexus injuries.1–3 Approximately 30% of posterior SCJ dislocations cause a life-threatening injury,14 with some meta-analyses finding much higher rates.15 Reduction of a posterior SCJ dislocation can release the pressure held on damaged structures, causing hemorrhage and decompensation as described further below.14,15 For this reason, closed reduction of posterior dislocations is generally done in the operating room with a thoracic surgeon present, although some orthopedic surgeons are comfortable managing these alone.1,2,26 Anterior dislocations, which do not share these complications, can be reduced in the emergency department (ED).1,2
Mechanism of Injury
SCJ dislocations are generally high-impact injuries due to its ligamentous strength.1–6 The most common causes are full-contact sports and motor vehicle injuries, with other causes being infrequent alternatives.1,2,16 Anterior dislocations generally result from forces to the posterior shoulder or to the lateral shoulder if held posteriorly.1,2,4 This occurs in part because the clavicle acts as a lever over the first rib in this position, promoting anterior dislocation. Impact to the lateral shoulder when the shoulder is held anteriorly can drive the medial clavicle under the manubrium, causing a posterior dislocation.1,2,4 In general, such dislocations are prevented as the clavicle fractures more readily than the ligaments rupture, dissipating the force, unless the impact is directed in line with the clavicular axis.16 Posterior dislocations can also be caused by a direct anterior blow to the medial clavicle.4 Rarely, SCJ dislocations can be caused by infection, rheumatologic disease, or occur spontaneously.2,7,17
Presentation
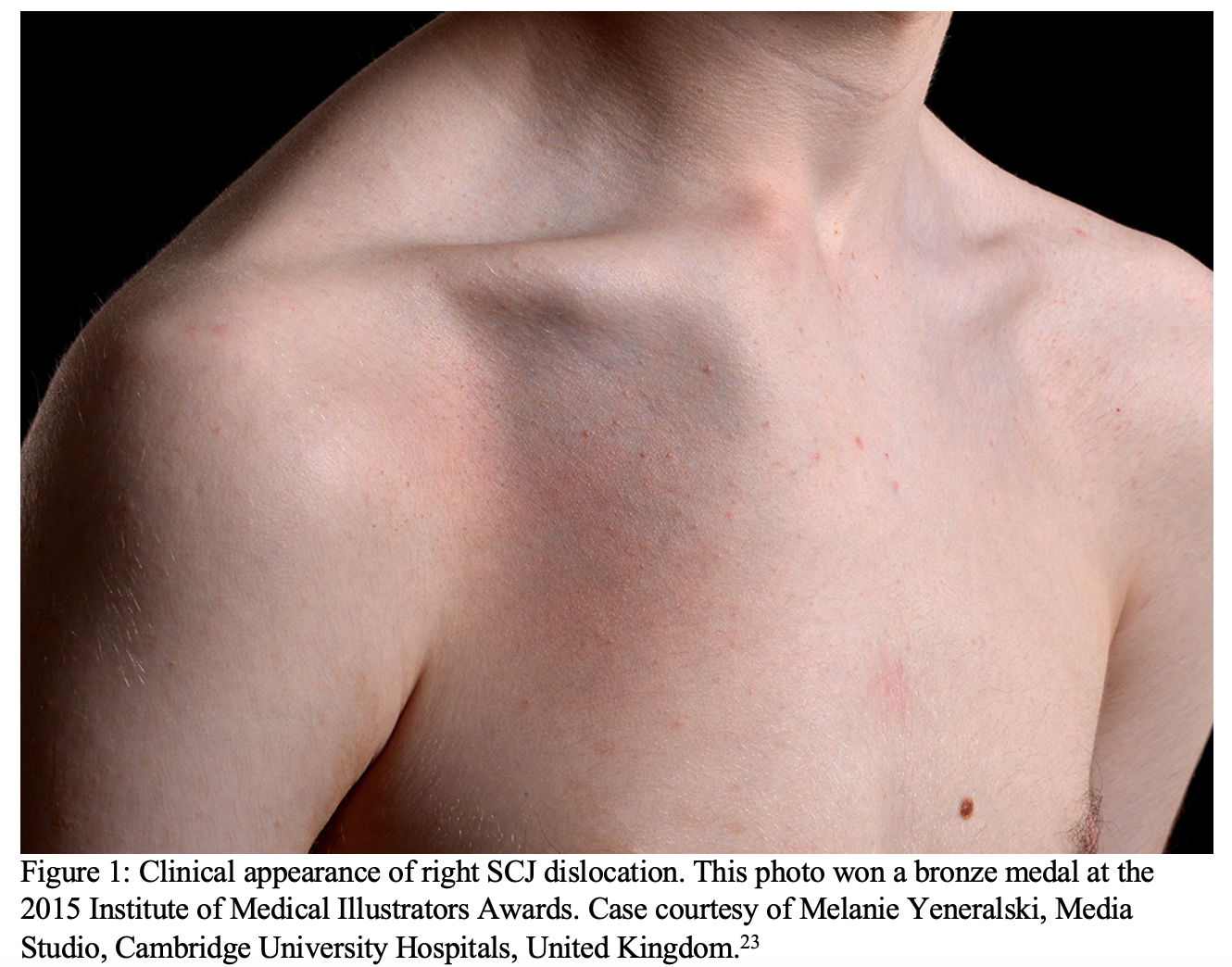
SCJ dislocations are extremely painful.1,2,4 As the SCJ participates in nearly all shoulder movements, patients generally hold the affected arm to stabilize the joint.1 Commonly, the affected arm will be flexed at the elbow, internally rotated, and supported by the opposite arm.1,4 The shoulder may appear more anterior and inferior than the unaffected shoulder.2,7 Patients with isolated anterior dislocations generally present with no other symptoms.16 Supine positioning often worsens symptoms, as does arm elevation and abduction.1,2,4 If internal structures are compromised, patients with posterior dislocations may present with symptoms related to the affected structure. Such patients may have hoarseness, stridor, dysphagia, dyspnea, diminished or absent ipsilateral upper extremity pulses, or ipsilateral upper extremity paresthesias and radiculopathy.1,2,4,18,19 Hypotension, hypoxia, tachycardia, and tachypnea can result from tracheal injuries, pneumothorax, and subclavian vessel damage. These signs and symptoms should prompt concern for posterior SCJ dislocation.1,2,4,18,19 In one report, a cervical murmur was auscultated secondary to brachiocephalic artery compression.18 In another, the brachiocephalic vein and superior vena cava were lacerated but tamponaded by the dislocated clavicle.19 Reduction in the ED would likely have resulted in catastrophe.19
Diagnosis
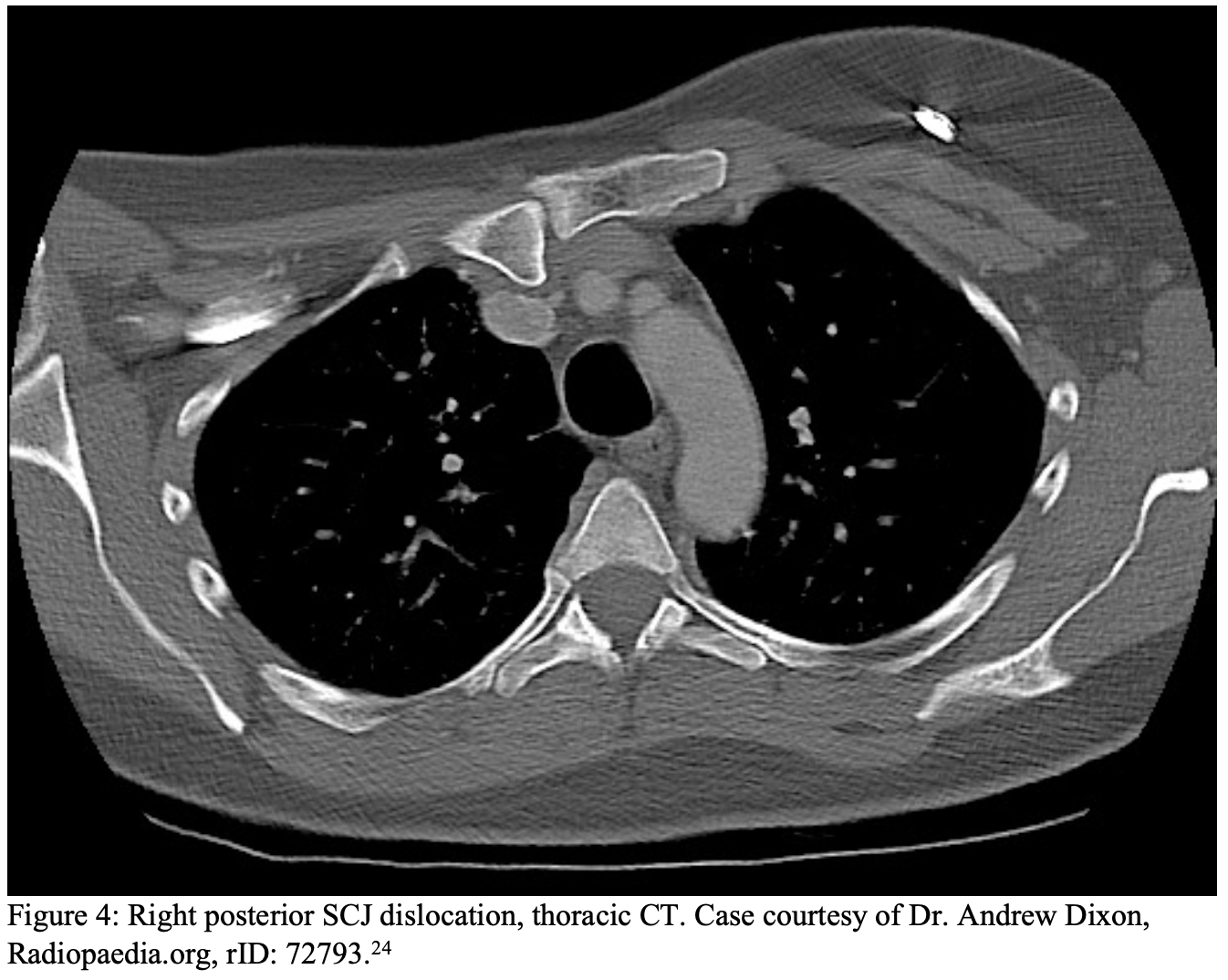
Physical exam cannot reliably distinguish between anterior and posterior dislocation, and imaging is necessary.4 The SCJ is poorly visualized on standard plain chest and shoulder films, which are often read as negative.1,4 Computed tomography (CT) imaging is the gold standard of diagnosis.1,4,20 If a posterior dislocation is suspected, obtain a CT chest angiogram to evaluate for vascular injury. Otherwise, a non-contrasted CT chest should suffice.1,2,4,7,13 The dense anatomy of the region prevents simple direct X-ray imaging parallel and perpendicular to the joint.4 However, if CT is unavailable, specialized plain films can be helpful. Take caution, however, as these can be challenging to interpret.1,4 Ultrasound can also be helpful as well, although it is rarely performed.21 The sensitivity and specificity of plain films, ultrasound, and CT for SCJ dislocation are unknown, although CT is universally recognized as superior.2,4,7,13
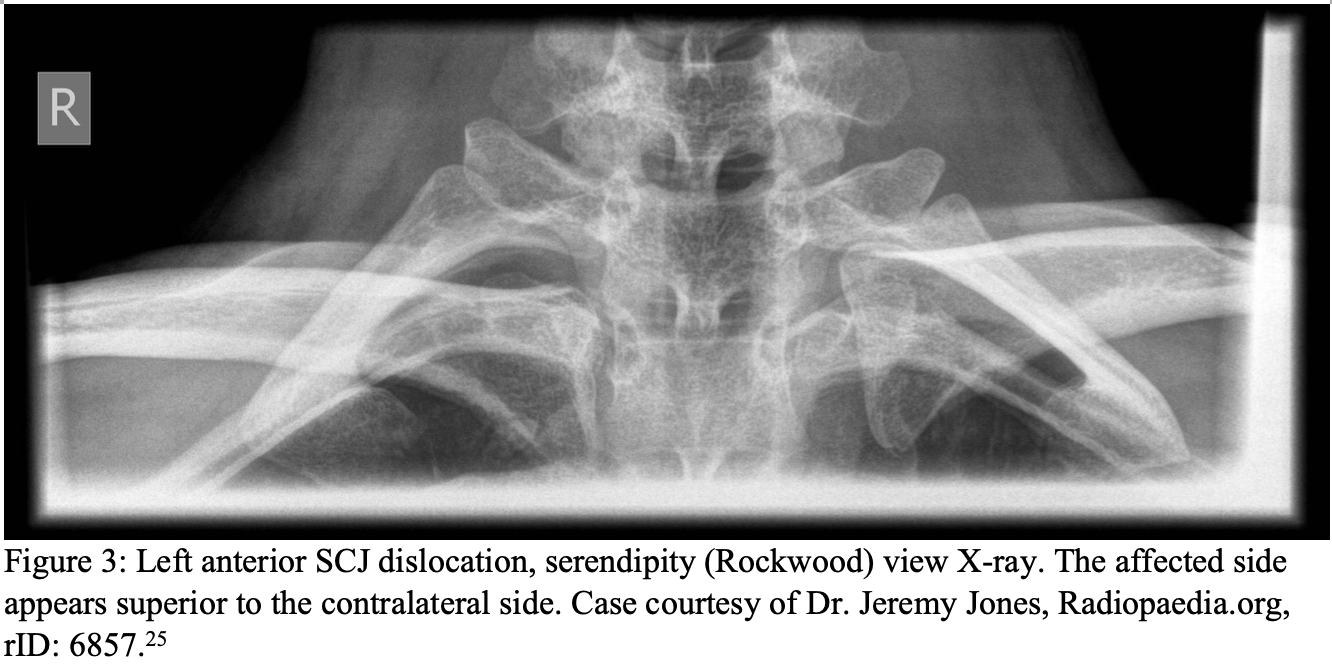
Although others have been proposed, the serendipity, lateral, and oblique views are the most common specialized X-ray views; these are also called the Rockwood, Heinig, and Hobbs views respectively.7,10 Both the serendipity and lateral views are anterior-posterior views obtained with the patient supine.4,7,10 The serendipity view (named for its accidental discovery) is centered on the SCJ with a 40° caudocephalic angle.4 In this view, the medial clavicle will appear depressed if posteriorly dislocated and elevated if anteriorly dislocated.10 For the lateral view, the beam is directed tangential to the joint, parallel to the opposite clavicle.4,10,22 The oblique view has the patient seated, bent over the detector with their flexed neck parallel to the table, and the beam directed from above onto the nape of the neck.4 The lateral and oblique views are rarely used in modern practice.1,2,4,7,10,22

Ultrasound of the SCJ is straightforward to perform with a high-frequency linear probe. Place the probe on the SCJ oriented along the clavicle. The clavicle should be roughly aligned with the manubrium in the anterior-posterior plane. A posterior SCJ dislocation will have the manubrium at its usual depth with the medial clavicle depressed, and an anterior SCJ dislocation will have the medial clavicle elevated. As point-of-care ultrasound of the SCJ is unfamiliar to most clinicians, comparison with the contralateral side is important to confirm asymmetry.21
Management
Acute SCJ subluxations and dislocations should be reduced, provided the patient presents within 10 days.1–4 All patients should be referred to orthopedics for follow-up. Subluxations can often be reduced by having the patient bring their shoulders back as if to touch the medial scapulae together. If this fails, attempt closed reduction as for anterior SCJ dislocation below.1–4 Patients with simple SCJ sprains should be placed in a sling for 4–5 days followed by gradual return to activity and ice as needed.2,4
Reduction of anterior SCJ dislocation usually fails but should be considered in the ED.3,4 Procedural sedation is usually necessary, but some patients tolerate closed reduction with local or no anesthesia.3,4 Place a 3–4” roll between the shoulder blades as the patient lies supine, then abduct the affected arm to approximately 90 degrees with mild extension so as to align the arm with the clavicle and apply traction.2,3 In this position, attempt to reduce the dislocation by direct pressure on the anteriorly-displaced medial clavicle. If this is unsuccessful, adduct the arm and apply traction, this time inferiorly, with direct pressure as before.26 However, given the instability of the ligamentously-disrupted SCJ, the joint easily dislocates again after reduction.4,17 If successful, keep the joint reduced with a pressure dressing, held in place by a figure-of-eight bandage or a bulky pad over the medial clavicle held with elastic rolls.4 If unsuccessful, preferentially use a figure-of-eight bandage or a sling and swath.1–4 A shoulder immobilizer is another option.1–4 The long-term management is generally benign neglect, and significant functional impairment is rare.1,2 However, some orthopedic surgeons do operate on selected patients, and all patients should be referred.27,28 Consulting orthopedics is not necessary for anterior dislocations but can be considered. Following reduction, patients should be immobilized for 4–6 weeks.
Posterior SCJ dislocations are high risk, as described above. Closed reduction becomes increasingly difficult 48 hours after injury, and chronic dislocations need no treatment.3,4 Acute posterior SCJ dislocations require emergency consultation to orthopedics and thoracic surgery. These usually require general anesthesia, although there are reports of reduction under procedural sedation or local anesthesia.1–6 Once reduced, these are generally stable, unlike anterior dislocations.3,4 Given their high risk, reductions in the ED should be attempted with extreme caution, but may be necessary if hemodynamic instability or airway compression results.1 In such a circumstance, position the patient as with anterior dislocations. Use the abduction and adduction methods as described above, but without direct pressure on the clavicle. If unsuccessful, an alternate technique uses a surgical towel clamp to grasp the clavicle and can be performed with the assistance of an orthopedic surgeon. Sterilize the skin with chlorhexidine or povidone iodine, then apply the towel clamp through the skin around (not into) the medial clavicle. Use great care with depth to avoid injuring the subclavian vessels. Attempt reduction as before, using the towel clamp to elevate and return the clavicle to its normal position.1-3 If unsuccessful, the patient will require surgery.1–3,15
Case Conclusions
- CT angiogram demonstrates a posterior SCJ dislocation with compression of the right subclavian artery. He is admitted to orthopedic surgery with thoracic surgery following for emergency reduction in the operating room.
- A serendipity view demonstrates an anterior SCJ dislocation. Closed reduction in the ED is successful but promptly re-dislocates. Her pain is controlled with oral analgesics. She is placed in a figure-of-eight bandage and discharged with orthopedics follow-up in 2 weeks.
Summary
- SCJ dislocations can be anterior or posterior.
- Strongly consider CT angiogram if posterior dislocation is suspected.
- Posterior SCJ dislocations can be life-threatening and are generally reduced in the OR.
- Immediate complications include tracheal, esophageal, and vessel damage.
- Late complications include persistent instability, chronic pain, and poor cosmesis.
On-shift Rapid Review
References
- Bengtzen RR and Daya MR. Shoulder. In Walls R, Hockberger R, Gausche-Hill M, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 9th ed. Philadelphia: Elsevier; 2018: 555–557.
- Hussain A and Malik S. Shoulder. In Sherman S, ed. Simon’s Emergency Orthopedics. 8th ed. New York: McGraw Hill; 2019: 356–359.
- Reichman EF. Sternoclavicular joint dislocation reduction. In Reichman EF, ed. Emergency Medicine Procedures. 2nd ed. New York: McGraw Hill; 2013: 526–531.
- Wirth MA, Rockwood CA. Acute and chronic traumatic injuries of the sternoclavicular joint. J Am Acad Orthop Surg. 1996; 4(5): 268–278. doi: 10.5435/00124635-199609000-00005
- Renfree KJ, Wright TW. Anatomy and biomechanics of the acromioclavicular and sternoclavicular joints. Clin Sports Med. 2003; 22(2): 219–237. doi: 10.1016/s0278-5919(02)00104-7
- Martetschläger F, Warth RJ, Millett PJ. Instability and degenerative arthritis of the sternoclavicular joint: a current concepts review. Am J Sports Med. 2014; 42(4): 999–1007. doi: 10.1177/036354651349899
- Robinson CM, Jenkins PJ, Markham PE, Beggs I. Disorders of the sternoclavicular joint. J Bone Joint Surg Br. 2008; 90(6): 685–696. doi: 10.1302/0301-620X.90B6.20391
- Groh GI, Wirth MA. Management of traumatic sternoclavicular joint injuries. J Am Acad Orthop Surg. 2011; 19(1): 1–7. doi: 10.5435/00124635-201101000-00001
- Tepolt F, Carry PM, Heyn PC, Miller NH. Posterior sternoclavicular joint injuries in the adolescent population: a meta-analysis. Am J Sports Med. 2014; 42(10): 2517–2524. doi: 10.1177/0363546514523386
- Cope R. Dislocations of the sternoclavicular joint. Skeletal Radiol. 1993; 22(4): 233–238. doi: 10.1007/bf00197665
- Meijerman L, Maat GJ, Schulz R, Schmeling A. Variables affecting the probability of complete fusion of the medial clavicular epiphysis. Int J Legal Med. 2007; 121(6): 463–468. doi: 10.1007/s00414-007-0189-z
- Ufuk F, Agladioglu K, Karabulut N. CT evaluation of medial clavicular epiphysis as a method of bone age determination in adolescents and young adults. Diagn Interv Radiol. 2016; 22(3): 241–246. doi: 10.5152/dir.2016.15355
- Yeh GL, Williams GR. Conservative management of sternoclavicular injuries. Orthop Clin North Am. 2000; 31(2):189–203. doi: 10.1016/s0030-5898(05)70140-1
- Ono K, Inagawa H, Kiyota K, Terada T, Suzuki S, Maekawa K. Posterior dislocation of the sternoclavicular joint with obstruction of the innominate vein: case report. J Trauma. 1998; 44(2): 381–383. doi: 10.1097/00005373-199802000-00027
- Kendal JK, Thomas K, Lo IKY, Bois AJ. Clinical outcomes and complications following surgical management of traumatic posterior sternoclavicular joint dislocations: a systematic review. JBJS Rev. 2018; 6(11): e2. doi: 10.2106/JBJS.RVW.17.00157
- Helman A, Sayal A, Dantzer D. Episode 136: Occult shoulder injuries and proximal humerus fractures. Emergency Medicine Cases. https://emergencymedicinecases.com/occult-shoulder-injuries-proximal-humerus-fractures. Published February 25, 2020. Accessed April 6, 2020: 29min – 35min.
- Morell DJ, Thyagarajan DS. Sternoclavicular joint dislocation and its management: a review of the literature. World J Orthop. 2016; 7(4): 244–250. doi: 10.5312/wjo.v7.i4.244
- Jougon JB, Lepront DJ, Dromer CEH. Posterior dislocation of the sternoclavicular joint leading to mediastinal compression. Ann Thorac Surg. 1996; 61(2): 711–713. doi: 10.1016/0003-4975(95)00745-8
- Worman LW, Leagus C. Intrathoracic injury following retrosternal dislocation of the clavicle. J Trauma. 1967; 7(3): 416–423.
- Sewell MD, Al-Hadithy N, Le Leu A, Lambert SM. Instability of the sternoclavicular joint: current concepts in classification, treatment and outcomes. Bone Joint J. 2013; 95-B(6): 721–731. doi: 10.1302/0301-620X.95B6.31064
- Bengtzen RR, Petering RC. Point-of-care ultrasound diagnosis of posterior sternoclavicular joint dislocation. J Emerg Med. 2017; 52(4): 513–515. doi: 10.1016/j.jemermed.2016.11.001
- Yang JS, Bogunovic L, Brophy RH, Wright RW, Scott R, Matava M. A case of posterior sternoclavicular dislocation in a professional American football player. Sports Health. 2015; 7(4): 318–325. doi: 10.1177/1941738113502153
- Yeneralski M. Dislocation of the sternoclavicular joint. Media Studio, Cambridge Biomedical Campus. Published 2015. Accessed April 21, 2020. http://www.media-studio.co.uk/about-us/awards
- El-Feky M, Jones J. Sternoclavicular joint dislocation. Radiopaedia. https://radiopaedia.org/articles/sternoclavicular-joint-dislocation. Published 2019. Accessed April 6, 2020.
- Deng F, Murphy A. Sternoclavicular joint (serendipity view). Radiopaedia. https://radiopaedia.org/articles/sternoclavicular-joint-serendipity-view. Published 2020. Accessed April 6, 2020.
- Buckerfield CT, Castle ME. Acute traumatic retrosternal dislocation of the clavicle. J Bone Joint Surg Am. 1984; 66(3): 379–385.
- Sernandez H, Riehl J. Sternoclavicular joint dislocation: a systematic review and meta-analysis. J Orthop Trauma. 2019; 33(7): e251– doi: 10.1097/BOT.0000000000001463
- Macdonald PB, Lapointe P. Acromioclavicular and sternoclavicular joint injuries. Orthop Clin North Am. 2008; 39(4): 535–545. doi: 10.1016/j.ocl.2008.05.003
- Weatherford B. Sternoclavicular dislocation. Orthobullets.https://www.orthobullets.com/trauma/1009/sternoclavicular-dislocation. Published March 4, 2019. Accessed April 6, 2020.
- Cadogan M. Sternoclavicular joint dislocation. Life in the Fast Lane. https://litfl.com/sternoclavicular-joint-dislocation. Published September 12, 2019. Accessed April 6, 2020.
- Astin M. Sternoclavicular joint dislocations: diagnosis and treatment. Academic Life in Emergency Medicine. https://www.aliem.com/sternoclavicular-joint-dislocations. Published July 21, 2014. Accessed April 6, 2020.




