Author: J. Daniel Ballew, DO (@dan_ballew, Global/Rural EM Health Fellow, University of Washington) // Edited by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit); Anthony DeVivo, DO (@anthony_devivo); and Manpreet Singh, MD (@MprizzleER)
Welcome back to the emDocs series, Unlocking Common ED Procedures! This series will provide key information on procedural steps, indications, contraindications, pearls, and pitfalls. This post looks at PTA drainage.

Check out our new downloadable procedure card with QR code link to the article. Print them out and be ready to go over it with your learners!
Case:
A 20-year-old female presents to the Emergency Department (ED) with 3 days of sore throat and pain with swallowing. Pain is worse on the left side of her throat. She has had multiple episodes of strep pharyngitis in the past but denies any other medical history. On exam, she is non-toxic appearing and in no distress, with mild trismus and a somewhat muffled voice. Examination of her oropharynx shows erythema and edema at the left peritonsillar pillar and uvular deviation to the right.
Background:
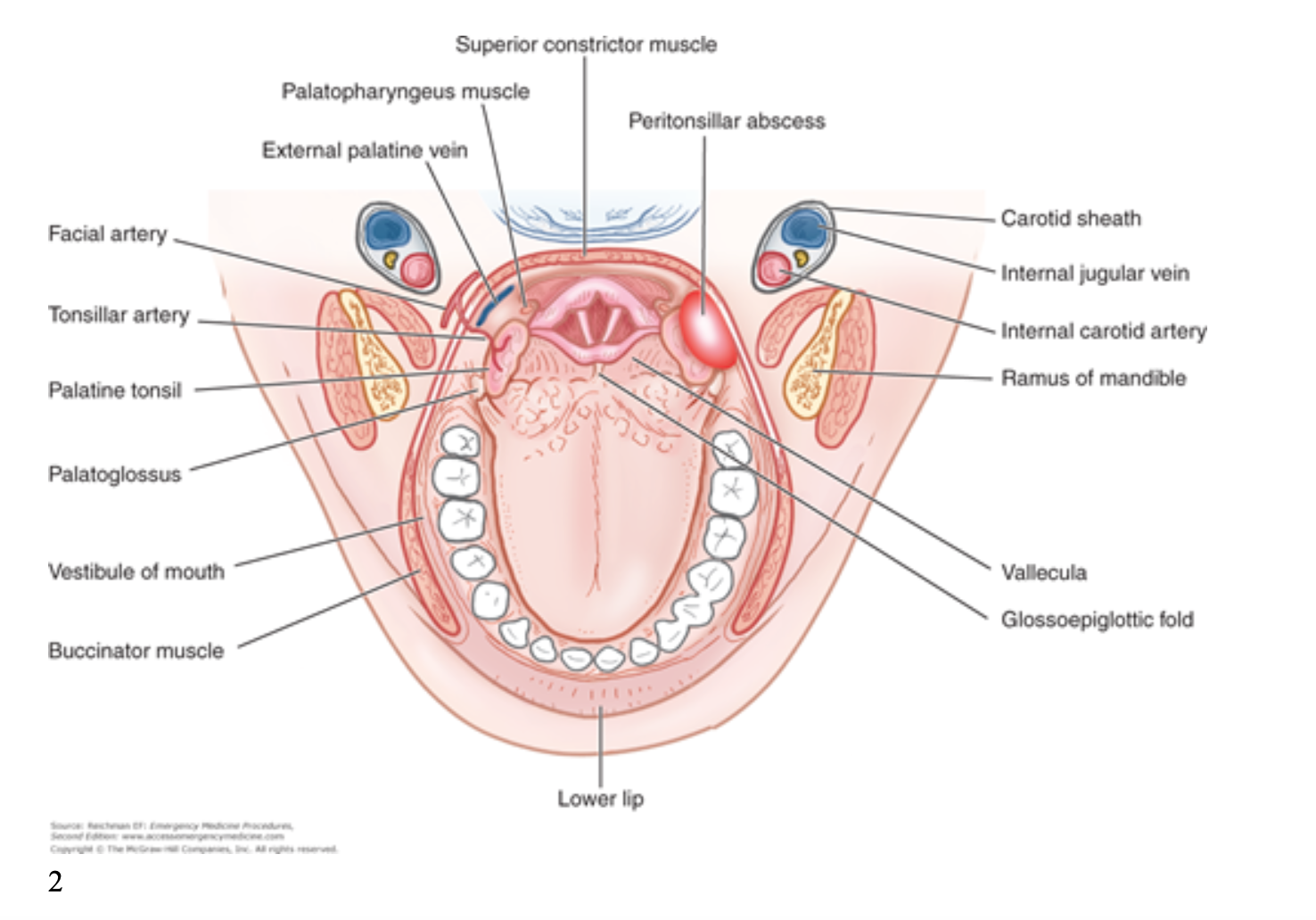
Peritonsillar abscess (PTA) is the most common deep space infection of the head and neck. Incidence has been estimated at 30 cases per 100,000 people in the U.S. annually¹. Diagnosis is generally made clinically with patients complaining of fever, sore throat, dysphonia, and odynophagia. The infection arises in the space between the palatine tonsil and the palatoglossal fold (figure 1). As you can see from the image below, the carotid is just posterior and lateral to this space.
PTA is predominantly a polymicrobial infection made up of oral flora³. CT as well as ultrasound (US) may be utilized to aid in diagnosis (more on US below). Management typically consists of drainage followed by a course of antibiotics. Antibiotics of choice include amoxicillin/clavulanate, penicillin, or clindamycin (or other antibiotic covering oral flora). Corticosteroids may aid in a faster recovery⁴. The studies for steroid use in PTA are somewhat limited, but a meta-analysis demonstrated slight improvement in pain and dysphagia at 24 hours after administration in patients who were given corticosteroids (methylprednisolone or dexamethasone; no studies have compared the two)⁵. All patients should follow up with ENT within 48 hours.
Indications and Contraindications:
The indication for drainage of PTA is diagnosis of PTA (pretty straightforward). At times diagnosis may be questionable, and further testing may be needed to confirm before attempting drainage. CT with intravenous contrast may be necessary in patients whose trismus is so severe that they cannot open their mouths wide enough for proper visualization, in cases when US results are equivocal, and with physician discretion. Contraindications of PTA drainage include severe trismus (so much so that intraoral visualization and instrumentation are limited), coagulopathy, and the uncooperative patient. If a patient is anticoagulated or has an inherited bleeding disorder, we recommend discussing with ENT before proceeding with drainage. With the uncooperative and anxious patient, one may attempt to discuss the procedure fully with the patient so he/she understands the full steps of the procedure, which can alleviate patient anxiety. Other patients may also benefit from benzodiazepine administration such as versed if there is severe anxiety related to the procedure.
Ultrasound in PTA:
Ultrasound can be a great aid in the diagnosis and drainage of PTA, and in one small study was superior to landmark-based diagnosis. In this study they utilized the intraoral approach and this led to more successful aspiration of purulent material, less use of CT scanning, and a smaller consult rate to ENT when compared to landmark diagnosis⁶. In another study, specificity and sensitivity of physical exam was 78% and 50%⁷. Intraoral and submandibular US have shown have shown a sensitivity and specificity of 80% to 95% and specificity of 78% to 100% in various studies⁷. This makes a strong argument for using US in aiding diagnosis of those suspected to have PTA. There are 2 possible approaches when using US in diagnosis and drainage of PTA: intraoral and submandibular.
Intraoral:
For the intraoral approach, the endocavitary probe is used. With a probe cover in place, the patient in a comfortable position, and preferably after the area is anesthetized, the probe is placed into the patient’s mouth and directed to the suspected location of abscess. It may be more comfortable for the patient if the probe is placed into the mouth themselves. When this is done, instruct the patient to softly place the end of the probe onto the area of greatest pain. This is generally the area of the abscess. Once the endocavitary probe is in place you may proceed with assessing for an abscess while also noting surrounding anatomic structures and their proximity to the abscess.
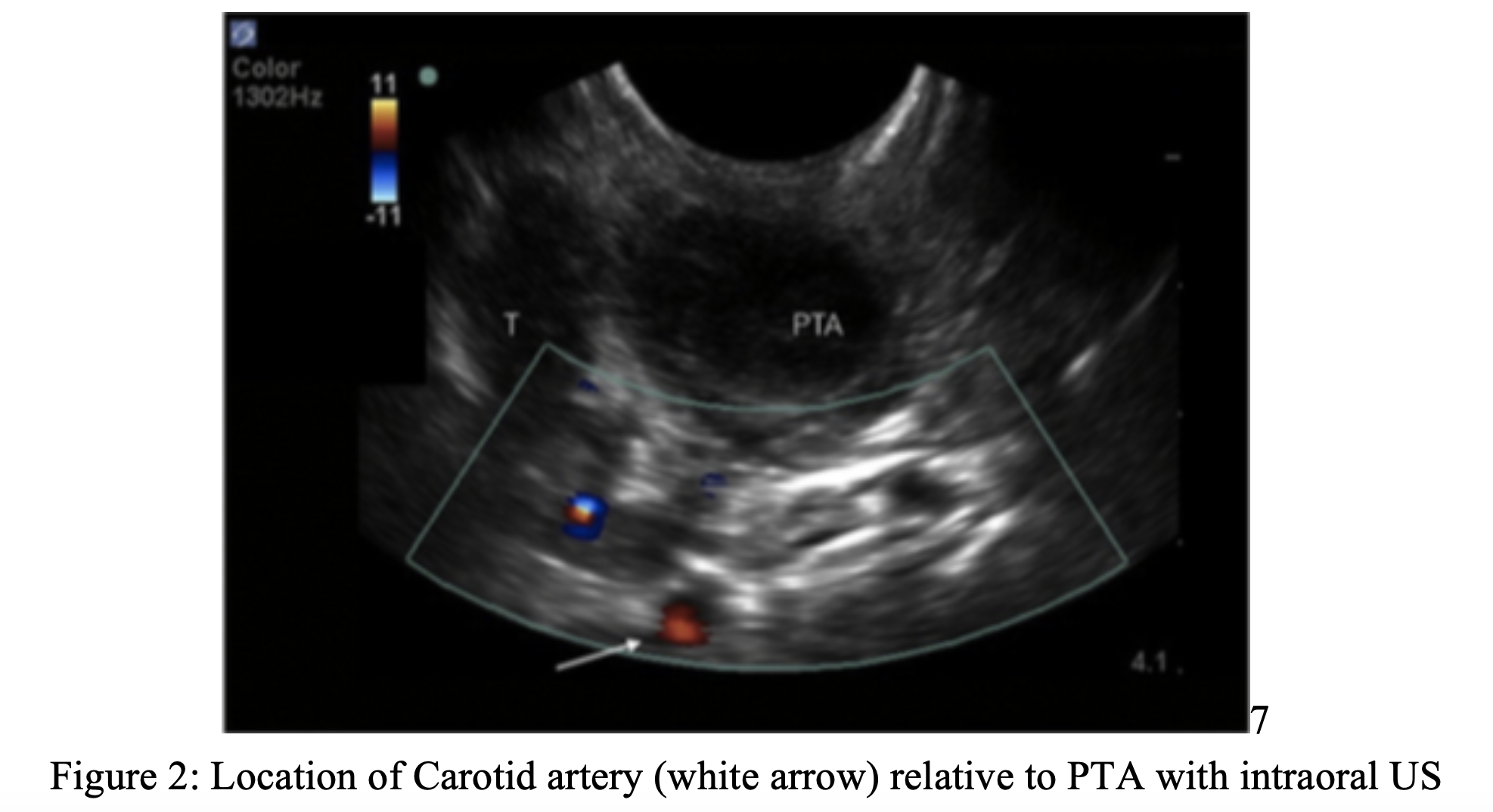
Submandibular:
Some patients may not be able to tolerate use of the intraoral US approach, secondary to trismus or discomfort (sometimes there just is not much space). An answer to this is the submandibular approach. Using the linear or curvilinear probe, place the probe just medial to the angle of the mandible on the side of the suspected PTA. The probe marker should be pointed towards the angle of the mandible. Fan the probe, looking for the abscess. If there is difficulty finding the abscess or tonsil, look for the carotid artery and jugular vein to assist with orientation⁷. This approach can be used for real-time US guided drainage of PTA. The video below discusses this further:
Procedure:
For PTA drainage, as in every procedure, setup is key. See the recommended equipment checklist below. The patient should be made comfortable. This is usually achieved by having the patient sit up with the back of their head resting on the bed or a pillow. Intravenous analgesia can assist⁸. Patients may need medication for anxiolysis pre-procedure as well. Take careful note of the patient’s response to medications administered as to not compromise respiratory drive. After intravenous medications have been given, anesthesia is obtained using a topical spray such as cetacaine or nebulized lidocaine. Remember, cetacaine comes with the possible risk of methemoglobinemia, but this is quite small⁹. Consider utilizing 4% nebulized lidocaine, using the mouthpiece nebulizer attachment instead of the mask so the medication is more concentrated to the desired area. Injecting a small amount of lidocaine with epinephrine into the area of abscess is also helpful to assess how well the area has been anesthetized after nebulization or spray. One may also consider glycopyrrolate use, as this may decrease secretions, but this has not been directly studied for this application.
Equipment Checklist for PTA Drainage:
- 18g spinal needle with sheath guard, with 1-1.5 cm of the needle left exposed
- 2, 10 cc syringes
- Size 11 blade scalpel with taped guard
- Size 3 or 4 Macintosh blade with handle
- Yankauer suction on continuous
- Curved hemostat
- Lidocaine with epinephrine
- Nebulizer set-up
- Patient on the monitor

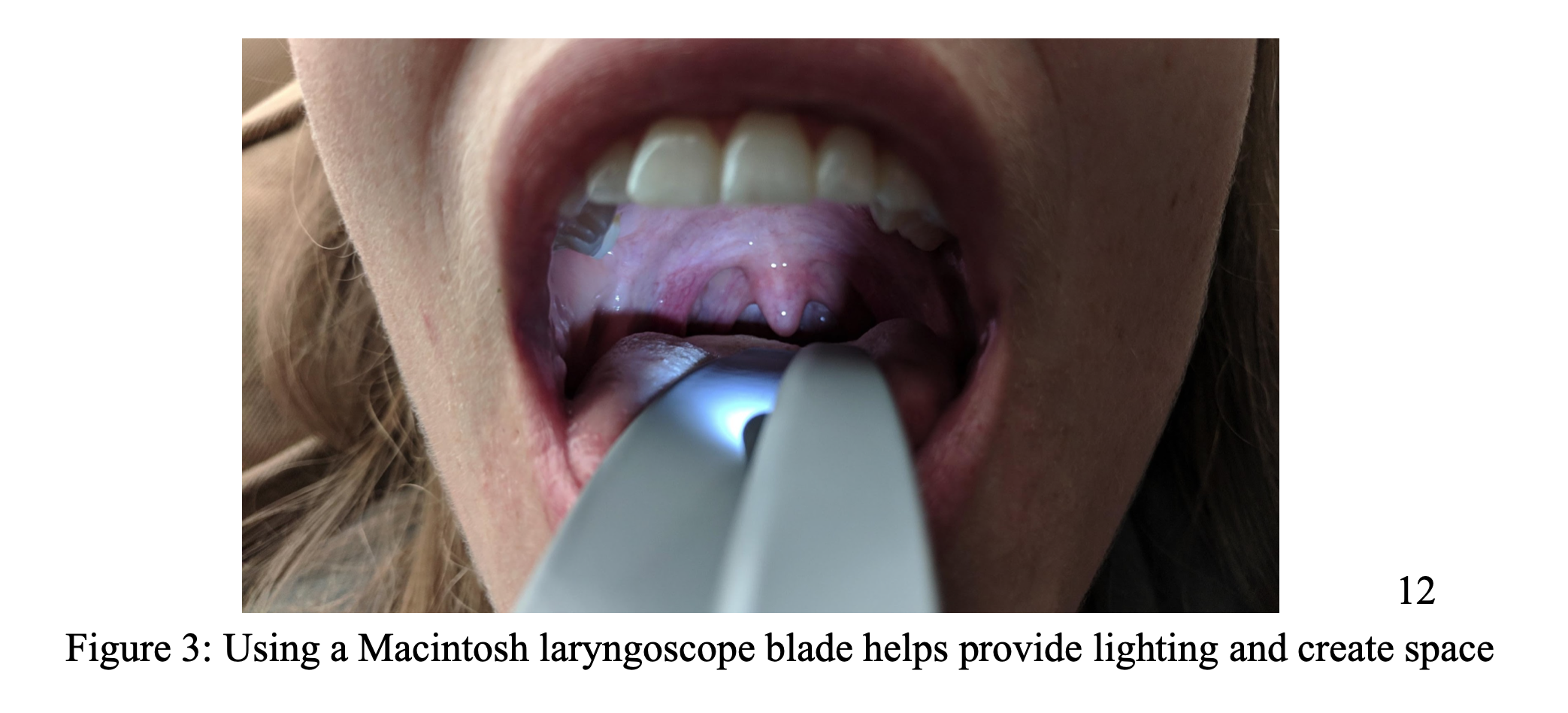
Once the patient is appropriately anesthetized, you may proceed with drainage. Insert the laryngoscope blade into the patient’s mouth to a depth that is comfortable for the patient but also allows adequate lighting and spacing for visualization of the abscess (figure 2). If the patient is comfortable to do so, it may be helpful to have him/her hold the laryngoscope in place. This allows the individual performing the procedure to have 2 free hands.
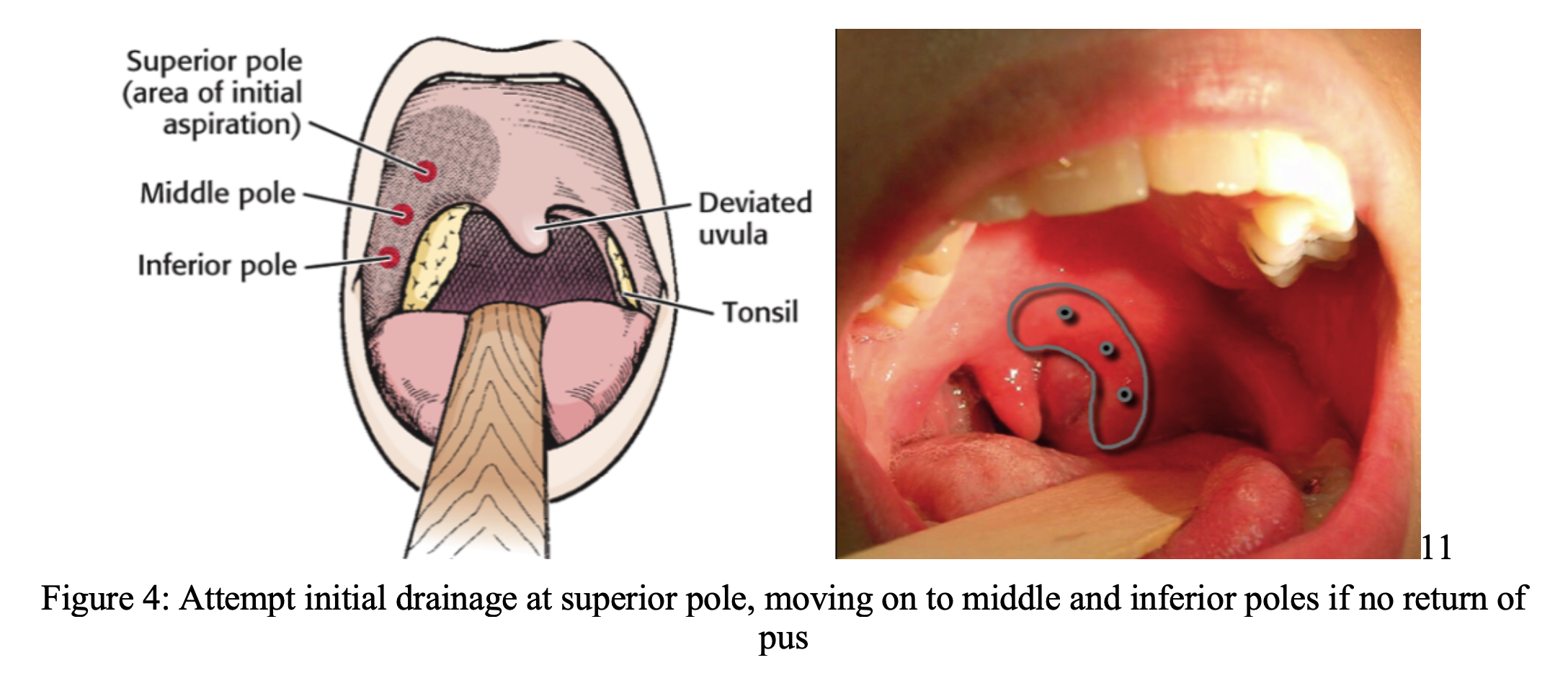
Once adequate visualization is achieved, approach the superior pole of the abscess with the sheathed spinal needle and continuously aspirate while advancing. If purulent drainage is obtained, remove as much pus as possible. If there is no purulent return at the superior pole, move on to the middle and inferior poles until there is return of pus. If there is a significant amount of pus obtained (around 5-6cc), you may consider incision with an #11 blade with taped guard. The approach for this is similar to using the spinal needle. Only stay and advance in the sagittal plane (remember Big Red is just posterolateral to your needle tip). After a single straight incision is made, you may attempt to break up any remaining loculations with a curved hemostat. We recommend using the scalpel only in fully cooperative patients.
There will likely be bleeding after the procedure. If there is a significant amount of bleeding, continued purulent drainage, or any other unforeseen complications, the patient may require admission. There are no specific guidelines for management of severe bleeding after PTA drainage. A general approach would be to manage the ABCs up front. Take the airway if necessary and prepare for a difficult, bloody airway. Apply direct pressure with TXA or lidocaine with epinephrine-soaked gauze¹⁰. This will likely be uncomfortable to the patient. ENT should be consulted swiftly in these cases.
Case Resolution:
The patient was diagnosed with peritonsillar abscess. She was anesthetized with nebulized lidocaine, and the abscess was drained using an 18g spinal needle with laryngoscope blade for visualization. 4cc of purulent drainage were obtained. Patient tolerated the procedure well. She was discharged on a course of amoxicillin/clavulanic acid. A follow up appointment was made with ENT for the following day.
Summary:
-Peritonsillar abscess is the most common deep space infection of the head and neck.
-Ultrasound can be used as an aid for diagnosis and location of PTA.
-Submandibular US is a useful approach for diagnosis and drainage in the patient with trismus.
-Initial approach of drainage is at the superior pole of the abscess, moving on to the middle and inferior poles as necessary.
-All patients should be sent home on antibiotics covering oral flora (amoxicillin/clavulanic acid, penicillin, clindamycin) and follow up with ENT within 48hrs.
Pearls and Pitfalls:
- No pus obtained from initial aspiration- Move on to the middle and inferior poles, palpate abscess to find area of greatest fluctuance and aim for this. Ultrasound the site to assess how much of a fluid collection is present.
- Trismus- Use the submandibular approach for visualization and drainage in mild to moderate trismus.
- Anxious patient- Talk about the procedure with the patient. Involve the patient in the procedure by holding the laryngoscope and suction. Administer small dose of IV anxiolysis such as versed or other short acting agents
- Consulting ENT- This will be institutionally based. Consider consulting in cases of significant bleeding, airway compromise, or severe trismus.
- Severe Bleeding- Evaluate and manage the ABCs. Consider taking the airway early. Apply direct pressure using Magill forceps and lidocaine with epinephrine or TXA soaked gauze. Nebulized TXA can be considered but this is a novel application of this medication.
Rapid Procedure Review:
- Once the diagnosis of PTA is suspected, use the submandibular or intraoral US approach to confirm diagnosis, assess the size of the abscess, and to see surrounding structures.
- When diagnosis is confirmed have all of your supplies brought to the bedside including 18g spinal needle and laryngoscope. Have suction ready.
- Use 4% lidocaine or another topical anesthetic to anesthetize the area.
- Once patient is comfortable, insert a laryngoscope blade to properly visualize the abscess.
- Insert the 18g spinal needle with guard into the superior pole of the abscess, moving to the middle and inferior poles if no purulent drainage is obtained at the superior pole.
- When there is no more purulent drainage remove the needle and laryngoscope blade. Observe the patient until bleeding has ceased.
- Once bleeding has ceased or slowed discharge the patient home with antibiotics covering oral flora (amoxicillin-clavulanate, clindamycin, etc.) and arrange ENT follow up within 48hrs.
References/Further Reading:
- Nicholas J. Galioto, MD, Broadlawns Medical Center, Des Moines, Iowa. Peritonsillar Abscess. Am Fam Physician. 2017 Apr 15;95(8):501-506. https://www.aafp.org/afp/2017/0415/p501.html
- Image courtesy of: https://accessemergencymedicine.mhmedical.com/content.aspx?bookid=683§ionid=45343823
- Emily L. Powell, Jason Powell, Julie R. Samuel, Janet A. Wilson; A review of the pathogenesis of adult peritonsillar abscess: time for a re-evaluation, Journal of Antimicrobial Chemotherapy, Volume 68, Issue 9, 1 September 2013, Pages 1941–1950, https://doi.org/10.1093/jac/dkt128
- Hur K, Zhou S, Kysh L; Adjunct steroids in the treatment of peritonsillar abscess: A systematic review. Laryngoscope. 2018 Jan;128(1):72-77. doi: 10.1002/lary.26672. https://www.ncbi.nlm.nih.gov/pubmed/28561258
- Yeon Ji Lee, Yeon Min Jeong, Ho Seok Lee, and Se Hwan Hwang. The Efficacy of Corticosteroids in the Treatment of Peritonsillar Abscess: A Meta-Analysis. Clin Exp Otorhinolaryngol. 2016 Jun; 9(2): 89–97. doi: 10.21053/ceo.2014.01851https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4881317/
- Costantino TG, Satz WA, Dehnkamp W, Goett H. Randomized trial comparing Intraoral ultrasound to landmark-based needle aspiration in patients with suspected peritonsillar abscess. Acad Emerg Med. 2012 Jun;19(6):626-31. doi: 10.1111/j.1553-2712.2012.01380.x.
- Secko M, Sivitz A, Think ultrasound first for peritonsillar swelling, Am J Emerg Med (2015), http://dx.doi.org/10.1016/ j.ajem.2015.01.031
- Riviello, Ralph J. Otolaryngologic Procedures. Roberts and Hedges’ Clinical Procedures in Emergency Medicine.Ed. James R. Roberts. Philadelphia, PA: Elsevier, 2014. 1303-1309.
- Chowdhary S, Bukoye B, Bhansali AM, et al. Risk of Topical Anesthetic–Induced Methemoglobinemia: A 10-Year Retrospective Case-Control Study. JAMA Intern Med.2013;173(9):771–776. doi:10.1001/jamainternmed.2013.75
- Fox, Sean M. Post-Tonsillectomy Hemorrhage. https://pedemmorsels.com/post-tonsillectomy-hemorrhage/. 2012
- Image courtesy of: https://hqmeded.com/peritonsillar-abscess-drainage/
- Image courtesy of: J. Daniel Ballew





2 thoughts on “Unlocking Common ED Procedures – Peritonsillar Abscess Drainage”
Great post thanks for sharing these pearls!
Pingback: Teaching Shifts: "Sore Throat" - County EM