Written by: Tim Montrief (@EMinMiami, EM Resident Physician, Jackson Memorial Health System), Jeffrey M. Scott (@jsemccm, Attending Physician, Jackson Memorial Health System), and Stephen Alerhand (@SAlerhand, Assistant Professor of Emergency Medicine, Rutgers New Jersey Medical School) // Edited By: Manpreet Singh, MD (@MPrizzleER – Assistant Professor of Emergency Medicine / Department of Emergency Medicine – Harbor-UCLA Medical Center) and Alex Koyfman, MD (@EMHighAK)
Background
Cardiac arrest is one of the most challenging presentations managed by emergency physicians. Stress, diagnostic uncertainty, and the time-sensitive nature of the presentation lead to challenging management decisions. However, following the wide dissemination of bedside transthoracic ultrasound, emergency physicians have used transthoracic echocardiography (TTE) for diagnosis, procedural guidance, and prognosis in patients with cardiac arrest [1-5]. While TTE has many benefits in the management of cardiac arrest, it is not without shortcomings. It has been associated with prolonged interruptions in chest compressions [6,7], provides inadequate imaging in up to half of critically ill patients [8], and may be obscured by body habitus, gastric insufflation, and defibrillator pad placement.
Conversely, transesophageal echocardiography (TEE) has been shown to provide adequate images in nearly all patients [9], and is easily performed by inserting the ultrasound probe into the esophagus to a typical depth of 19-20 cm [10]. Laryngoscopy is not required for TEE placement, although if the patient’s airway is already secured via endotracheal intubation, the probe is more easily directed into the esophagus. The controls and handle, similar in nature to a bronchoscope, allow the physician to manipulate the transducer for myriad cardiac views similar in nature to those of TTE.
Transesophageal compared to transthoracic echocardiography
TEE obtains higher-resolution images compared to TTE, as the transducer lies only millimeters from the heart and is not affected by the patient’s body habitus, defibrillator pads, subcutaneous air, or lung disease. Additionally, TEE provides constant visualization of the heart throughout resuscitation, allowing simultaneous feedback on the efficacy of interventions (infusion of inotropes, cardioversion, pericardiocentesis, pneumothorax decompression, etc.), cardiac contractility, and compression quality [11,12]. Likewise, TEE is an invaluable adjunct in the determination and treatment of reversible causes of cardiac arrest including myocardial infarction, pulmonary embolism, pericardial tamponade, tension pneumothorax, and hypovolemia. Within the anesthesia literature, TEE has been shown to reliably identify the cause of intra-operative arrest as often as 86% of the time [13]. Although pharyngeal and esophageal laceration or hematoma can occur, TEE is relatively safe [14]. The most dangerous complication of TEE placement is esophageal perforation, with an incidence of roughly 0.03% [15]. Potential contraindications to TEE use include placement of a supraglottic airway, perforated viscus, esophagectomy, esophageal stricture, and massive upper gastrointestinal bleeding [16,17].
Transesophageal echo protocols
There remains no consensus TEE protocol for use during cardiac arrest, although many have been developed and investigated [18-22]. Within the anesthesia literature, a comprehensive intraoperative TEE examination may consist of up to 28 view [23]. However, The American College of Emergency Physicians (ACEP) released a clinical policy on TEE in cardiac arrest in 2017 which provides some guidance in regards to the specifications of individual examinations [24]. In cardiac arrest, a less complex protocol is needed to adequately investigate common pathologies and provide procedural guidance. The ACEP-recommended imaging sequence is designed for efficiency and represents the minimum standard of care for TEE in emergency department (ED) cardiac arrest patients, and allows for a variety of probe manipulations [25]. This sequence adheres to important principles of TEE in the ED, including:
- Utilizing views that are anatomically familiar and relatable to commonly used TTE views
- The need for efficiency and simplicity
- The need for redundancy to corroborate important findings across multiple planes of interrogation [26]
The most common and useful TEE views and their corresponding TTE views are below [27] (Fig 1):
TEE clips courtesy of Drs. Atif Qasim and Amresh Raina, http://www.echocardiographer.org. TEE images adapted from Arntfield R, Pace J, McLeod S, et al. Focused transesophageal echocardiography for emergency physicians-description and results from simulation training of a structured four-view examination. Crit Ultrasound J. 2015;7(1):27. TTE images from https://radiologykey.com/transthoracic-echocardiography-an-overview/ and https://web.stanford.edu/group/ccm_echocardio/cgi-bin/mediawiki/index.php/Subcostal_inferior_vena_cava_view
Midesophageal four chamber view
The midesophageal 4-chamber view (Fig. 2) is the most intuitive view to obtain, and is similar in nature to the common TTE apical four chamber view. This view is obtained by advancing the TEE probe to the thoracic esophagus and orienting the multiplane at 0-20° in neutral flexion, after which all four chambers can be visualized. This view provides excellent visualization of both ventricles and atria as well as the tricuspid and mitral valves in the same plane. It is important to avoid foreshortening the ventricles, and mild retroflexion of the probe is sometimes necessary. This view is useful for evaluation of right and left ventricular systolic function as well as size, and is the preferred view to evaluate for the presence or absence of a perfusing rhythm during a pulse check.
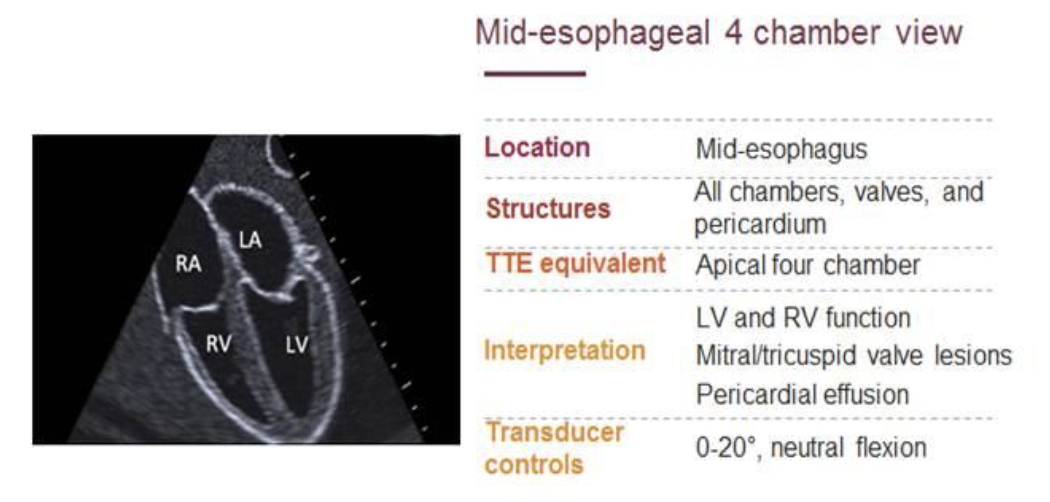
Figure 2: Mid-esophageal 4-chamber view
Adapted from Arntfield R, Pace J, McLeod S, et al. Focused transesophageal echocardiography for emergency physicians-description and results from simulation training of a structured four-view examination. Crit Ultrasound J. 2015;7(1):27.
Midesophageal Long Axis view
The midesophageal long-axis view (Fig. 3) is analogous to the parasternal long axis view in TTE, and is obtained by leaving the probe in the same location as the midesophageal 4-chamber, but increasing the multiplane to between 110° and 160° while in neutral flexion. This view includes the mitral and aortic valves, as well as the left atrium, left ventricle, and left ventricular outflow tract of the right ventricle. This view allows the physician to evaluate left ventricular systolic function, and provides real-time feedback on compression adequacy and location. High-quality compressions cause maximal compression of the left ventricle and subsequent opening of the aortic valve.

Figure 3: Mid-esophageal long axis view
Adapted from Arntfield R, Pace J, McLeod S, et al. Focused transesophageal echocardiography for emergency physicians-description and results from simulation training of a structured four-view examination. Crit Ultrasound J. 2015;7(1):27.
Transgastric Short Axis view
The transgastric short axis (Fig. 4) is analogous to the parasternal short axis TTE view, and is obtained by first moving the multiplane to 0°, then advancing the probe into the stomach and anteflexing the probe in order to view the left ventricle and right ventricle in cross-section. Of note, compared to the TTE parasternal short axis view, the location of the inferior wall is closest to probe in the TEE transgastric short axis. This view allows the operator to evaluate left ventricular systolic function, including any regional wall motion abnormalities suggestive of acute myocardial infarction, and the presence of septal flattening representing increased right ventricular pressures.

Figure 4: Trans-gastric short axis view
Adapted from Arntfield R, Pace J, McLeod S, et al. Focused transesophageal echocardiography for emergency physicians-description and results from simulation training of a structured four-view examination. Crit Ultrasound J. 2015;7(1):27.
Bicaval View
The bicaval view (Fig. 5) is most similar to the inferior vena cava view of TTE, and is obtained by turning the entire probe to the patient’s right towards the superior vena cava (SVC) and inferior vena cava (IVC) while in the midesophagus, keeping the multiplane at 90-100° with neutral flexion. The transducer plane cuts through the left atrium (LA), right atrium (RA), IVC and SVC. This view allows the operator to evaluate for hypovolemia, atrial size, and interatrial septum bowing. Additionally, the bicaval view aids in the placement of central venous catheters, transvenous pacemakers, or extracorporeal life support (ECMO) vascular cannulas by observing the initial wire placement in the vasculature [28].

Figure 5: Bicaval view
Adapted from Arntfield R, Pace J, McLeod S, et al. Focused transesophageal echocardiography for emergency physicians-description and results from simulation training of a structured four-view examination. Crit Ultrasound J. 2015;7(1):27.
Cases
Case 1 is adapted from clips from the University of Washington Department of Anesthesia’s transesophageal echocardiogram of the month, courtesy of Dr. Donald Oxorn.
Case 1: A 70-year-old male arrives after an out of hospital cardiac arrest. According to EMS, he was eating breakfast when he suddenly clutched his chest. On EMS arrival, he was ashen, in severe respiratory distress and cardiogenic shock. A 12-lead EKG showed an anterior wall STEMI. On the way to the hospital, he went into cardiac arrest. After 10 minutes of chest compressions, intubation, and epinephrine administration, he is still in pulseless electrical activity. You perform a TEE and see the following.
Midesophageal long axis

Transgastric short axis

As can be seen in both clips, the left ventricle demonstrates a severely depressed contractility. The patient appears to have organized cardiac rhythm, with a pulse that cannot be appreciated on physical exam.
Case 2 is adapted from clips from the Duke Department of Anesthesia’s transesophageal echocardiogram interesting case series, courtesy of Dr. Emily Teeter and Dr. Christopher Rigsby.
A 20-year-old male arrives in cardiac arrest. According to EMS, he was playing basketball when he suddenly clutched his chest and lost consciousness. On EMS arrival, he was cold, in severe respiratory distress and cardiogenic shock. A 12-lead EKG showed sinus tachycardia. On the way to the hospital, he went into cardiac arrest. After 15 minutes of chest compressions, intubation, and epinephrine administration, he is still in pulseless electrical activity. You perform a TEE and see the following
Midesophageal 4 chamber view, with color flow

Midesophageal long axis view with color

This patient has a large myxoma in his left atrium intermittently obstructing his mitral valve. On TEE, myxomas usually appear as sessile or pedunculated heterogeneous structures and are most commonly attached by a stalk to the interatrial septum in the left atrium. Mxyomas may prolapse through the atrioventricular valve and can cause obstruction or damage to the valve, such as the case with this patient.
Case 3 is adapted from clips courtesy of Dr. Stephen Alerhand
A 65-year-old male arrives to the emergency department with a chief complaint of central chest pressure for the previous 3 hours. As you are taking a further history, he goes into cardiac arrest. After 5 minutes of chest compressions, intubation, defibrillations, and epinephrine administration, he is still in ventricular fibrillation. You perform a TEE and see the following.
Midesophageal long axis view

Midesophageal four chamber view

Transgastric view

After 45 minutes of high quality chest compressions, you see the following:
Midesophageal long axis view

In the first three clips, there appears to be suboptimal cardiac output generated by cardiac compressions. This is evidenced by the lack of aortic valve opening during compressions, and the overall suboptimal squeeze of the LV. This information can be used to optimize the quality of chest compresions during resuscitation, as well as their location on the chest. In the follow up TEE, there is obvious blood pooling in all chambers, with agonal cardiac activity.
Training and credentialing in transesophageal echo
The American College of Emergency Physicians released a clinical policy on TEE in cardiac arrest in 2017, detailing the qualifications and responsibilities of the TEE performer, as well as individual TEE examination specifications, documentation, equipment specifications, and quality control. TEE credentialing is a question of technical ability and image acquisition, as providers achieve adequate image interpretation through credentialing in TEE [23]. Within the literature, there is evidence showing that performing as few as 10 examinations is adequate to establish competency for a limited examination, and there are a variety of simulation technologies available to supplement training [29-33]. Likewise, there are templates for standardized direct observation tool for TEE proctoring [26].
Future of TEE
Although the current focus of TEE is on cardiac arrest in the ED, its usefulness could soon extend to other critically ill patients during resuscitation.TEE would be an alternative to TTE (in those patients with poor windows) in determining the cause of shock, assessing fluid responsiveness, and continuously monitoring patients during resuscitation [33]. Likewise, in patients with atrial fibrillation, TEE could provide adequate examination of the left atrial appendage, subsequently followed by cardioversion if no thrombus is found, and may provide an alternative approach to inpatient admission. With regards to procedural guidance, TEE can help ensure the proper placement of intra-aortic balloon pumps, ECMO cannulas, transvenous pacemakers, and resuscitative intravascular devices including resuscitative endovascular balloon occlusion of the aorta (REBOA).
Pearls and Pitfalls
- TEE provides high-resolution images continually throughout resuscitation without causing prolonged interruptions in chest compressions, and is not distorted by the patient’s body habitus, defibrillator pads, subcutaneous air, or lung disease.
- TEE is an invaluable tool in the investigation and treatment of reversible causes of cardiac arrest including myocardial infarction, pulmonary embolism, pericardial tamponade, tension pneumothorax, and hypovolemia.
- Complications of TEE are rare, but include pharyngeal and esophageal laceration, hematoma, or esophageal perforation.
- The most common and useful TEE views include the midesophageal four chamber, midesophageal long axis, transgastric short axis, and bicaval views, which are analogous to common TTE views (apical four chamber, parasternal long axis, parasternal short axis, and subcostal IVC, respectively).
- ACEP has provided a clinical policy recommending the following for competency standards: 1) minimum of 2–4 hours of TEE specific training or education, 2) performing at least 10 proctored TEE examinations in live patients and simulation models, and 3) completion of a standardized assessment by a credentialed TEE provider.
References
- Blyth L., Atkinson P., Gadd K., et al: Bedside focused echocardiography as predictor of survival in cardiac arrest patients: a systematic review. Acad Emerg Med 2012; 19: pp. 1119-1126
- Breitkreutz R., Price S., Steiger H.V., et al: Focused echocardiographic evaluation in life support and peri-resuscitation of emergency patients: a prospective trial. Resuscitation 2010; 81: pp. 1527-1533
- Zengin S., Erdal Y., Al B., et al: Benefits of cardiac sonography performed by a non-expert sonographer in patients with non-traumatic cardiopulmonary arrest. Resuscitation 2016; 102: pp. 105-109
- Gaspari R., Weekes A., Adhikari S., et al: Emergency department point-of-care ultrasound in out-of-hospital and in-ED cardiac arrest. Resuscitation 2016; 109: pp. 33-39
- Hernandez C., Shuler K., Hannan H., et al: C.A.U.S.E.: cardiac arrest ultra-sound exam—a better approach to managing patients in primary non-arrhythmogenic cardiac arrest. Resuscitation 2008; 76: pp. 198-206
- Huis In’t Veld M.A., Allison M.G., Bostick D.S., et al: Ultrasound use during cardiopulmonary resuscitation is associated with delays in chest compressions. Resuscitation 2017 Oct; 119: pp. 95-98
- Clattenburg E.J., Wroe P., Brown S., et al: Point-of-care ultrasound use in patients with cardiac arrest is associated prolonged cardiopulmonary resuscitation pauses: a prospective cohort study. Resuscitation 2017 Nov 23; 122: pp. 65-68
- Parker M.M., Cunnion R.E., and Parrillo J.E.: Echocardiography and nuclear cardiac imaging in the critical care unit. JAMA 1985; 254: pp. 2935-2939
- Vignon P, Mentec H, Terré S, et al. Diagnostic accuracy and therapeutic impact of transthoracic and transesophageal echocardiography in mechanically ventilated patients in the ICU. Chest. 1994;106(6):1829–1834. doi: 10.1378/chest.106.6.1829.
- Kothavale A.A., Yeon S.B., and Manning W.J.: A systematic approach to performing a comprehensive transesophageal echocardiogram. A call to order. BMC Cardiovasc Disord 2009; 9: pp. 18
- van der Wouw P.A., Koster R.W., Delemarre B.J., et al: Diagnostic accuracy of transesophageal echocardiography during cardiopulmonary resuscitation. J Am Coll Cardiol 1997 Sep; 30: pp. 780-783
- Hwang S.O., Zhao P.G., Choi H.J., et al: Compression of the left ventricular outflow tract during cardiopulmonary resuscitation. Acad Emerg Med 2009 Oct; 16: pp. 928-933
- Memtsoudis S.G., Rosenberger P., Loffler M., et al: The usefulness of transesophageal echocardiography during intraoperative cardiac arrest in noncardiac surgery. Anesth Analg 2006; 102: pp. 1653-1657
- Aviv J.E., Di Tullio M.R., Homma S., et al: Hypopharyngeal perforation near-miss during transesophageal echocardiography. Laryngoscope 2004; 114: pp. 821-826
- MacGregor D.A., Zvara D.A., Treadway B.M., et al: Late presentation of esophageal injury after transesophageal echocardiography. Anesth Analg 2004; 99: pp. 41-44
- Daniel W.G., Erbel R., Kasper W., et al: Safety of transesophageal echocardiography. A multicenter survey of 10,419 examinations. Circulation 1991; 83: pp. 817-821
- Gendreau M.A., Triner W.R., and Bartfield J.: Complications of transesophageal echocardiography in the ED. Am J Emerg Med 1999; 17: pp. 248-251
- Byars DV, Tozer J, Joyce JM, et al. Emergency Physician-performed Transesophageal Echocardiography in Simulated Cardiac Arrest. West J Emerg Med. 2017;18(5):830-834.
- Arntfield R, Pace J, Hewak M, Thompson D. Focused Transesophageal Echocardiography by Emergency Physicians is Feasible and Clinically Influential: Observational Results from a Novel Ultrasound Program. J Emerg Med. 2016;50(2):286-94.
- Arntfield R, Pace J, McLeod S, et al. Focused transesophageal echocardiography for emergency physicians-description and results from simulation training of a structured four-view examination. Crit Ultrasound J. 2015;7(1):27.
- Rebel A, Klimkina O, Hassan ZU. Transesophageal echocardiography for the noncardiac surgical patient. Int Surg. 2012;97(1):43-55.
- Arntfield R, Pace J, Mcleod S, Granton J, Hegazy A, Lingard L. Focused transesophageal echocardiography for emergency physicians-description and results from simulation training of a structured four-view examination. Crit Ultrasound J. 2015;7(1):27.
- Staudt GE, Shelton K. Development of a Rescue Echocardiography Protocol for Noncardiac Surgery Patients. Anesth Analg. 2018. [Epub ahead of print]
- ACEP Board of Directors : Guidelines for the use of transesophageal echocardiography (TEE) in the ED for cardiac arrest. Ann Emerg Med 2017; 70: pp. 442-445
- Shanewise J.S, Cheung A.T, Aronson S, Stewart W.J, Weiss R.L, Mark J.B, et al. ASE/SCA guidelines for performing a comprehensive intraoperative multiplane transesophageal echocardiography examination: recommendations of the American Society of Echocardiography Council for Intraoperative Echocardiography and the Society of Cardiovascular Anesthesiologists Task Force for Certification in Perioperative Transesophageal Echocardiography. Anesth Analg. 1999;89(4):870–884.
- Fair J, Mallin M, Mallemat H, et al. Transesophageal Echocardiography: Guidelines for Point-of-Care Applications in Cardiac Arrest Resuscitation. Ann Emerg Med. 2018;71(2):201-207.
- Blaivas M.: Transesophageal echocardiography during cardiopulmonary arrest in the emergency department. Resuscitation 2008; 78: pp. 135-140
- Fair J, Tonna J, Ockerse P, et al: Emergency physician–performed transesophageal echocardiography for extracorporeal life support vascular cannula placement. Am J Emerg Med 2016; 34: pp. 1637-1639
- Matyal R, Montealegre-Gallegos M, Mitchell JD, et al. Manual skill acquisition during transesophageal echocardiography simulator training of cardiology fellows: a kinematic assessment. J Cardiothorac Vasc Anesth. 2015;29(6):1504–10.
- Sharma V, Chamos C, Valencia O, et al. The impact of internet and simulation-based training on transoesophageal echocardiography learning in anaesthetic trainees: a prospective randomised study. Anaesthesia. 2013;68(6):621–7.
- Jelacic S, Bowdle A, Togashi K, et al. The use of TEE simulation in teaching basic echocardiography skills to senior anesthesiology residents. J Cardiothorac Vasc Anesth. 2013;27(4):670–5.
- Sohmer B, Hudson C, Hudson J, et al. Transesophageal echocardiography simulation is an effective tool in teaching psychomotor skills to novice echocardiographers. Can J Anaesth. 2013;61(3):235–41.
- Damp J, Anthony R, Davidson MA, et al. Effects of transesophageal echocardiography simulator training on learning and performance in cardiovascular medicine fellows. J Am Soc of Echocardiogr. 2013;26(12):1450–6.
- Mayo PH, Narasimhan M, Koenig S. Critical Care Transesophageal Echocardiography. Chest. 2015;148(5):1323-1332.





2 thoughts on “US Probe: Transesophageal Echocardiography in Cardiac Arrest”
Pingback: LITFL Review 343 • LITFL
Pingback: Länkar v42-43 | Internmedicin