
Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK)

The American Heart Association 2023 Guideline for managing cardiac arrest or life-threatening toxicity due to poisoning was recently released. This post will focus on the key parts of the guideline that affect ED evaluation and management.
Top 10 Take Home Pearls
1. Treatment of cardiac arrest and life-threatening toxicity due to poisoning often requires specialized treatments that most clinicians do not use frequently such as antidotes and venoarterial extracorporeal membrane oxygenation, in addition to effective basic and advanced life support. Timely consultation with a medical toxicologist, clinical toxicologist, or regional poison center facilitates rapid and effective therapy.
2. Opioid overdose remains the leading cause of cardiac arrest due to poisoning in North America. Naloxone administration may reverse respiratory arrest, preventing progression to cardiac arrest.
3. High-dose insulin therapy is recommended early in the treatment of patients with life-threatening β-blocker and calcium channel blocker poisoning.
4. Standard advanced life support with the addition of administration of sodium bicarbonate is appropriate for the treatment of life-threatening dysrhythmias caused by cocaine or other sodium channel blockers.
5. If cyanide poisoning is suspected, do not wait for confirmatory testing. Treat immediately with hydroxocobalamin (preferred) or sodium nitrite plus sodium thiosulfate.
6. Administration of digoxin-specific immune antibody fragments can reverse life-threatening dysrhythmias from digoxin poisoning.
7. Use of 20% intravenous lipid emulsion can be efficacious in the resuscitation of life-threatening local anesthetic toxicity, especially from bupivacaine.
8. Patients with severe agitation from sympathomimetic poisoning require sedation to manage hyperthermia and acidosis, to prevent rhabdomyolysis and injury, and to allow evaluation for other life-threatening conditions.
9. Flumazenil reverses central nervous system and respiratory depression from benzodiazepine poisoning, but important risks and contraindications limit its use.
10. Venoarterial extracorporeal membrane oxygenation can be lifesaving for patients with cardiogenic shock or dysrhythmias that are refractory to other treatment measures. Because venoarterial extracorporeal membrane oxygenation implementation takes time, the process should be started early in patients who are not responding well to other therapies.
The Recommendations
All recommendations are designated with a class of recommendation (COR) and level of evidence (LOE). COR is the strength of the recommendation, while the LOE is the quality of scientific evidence.

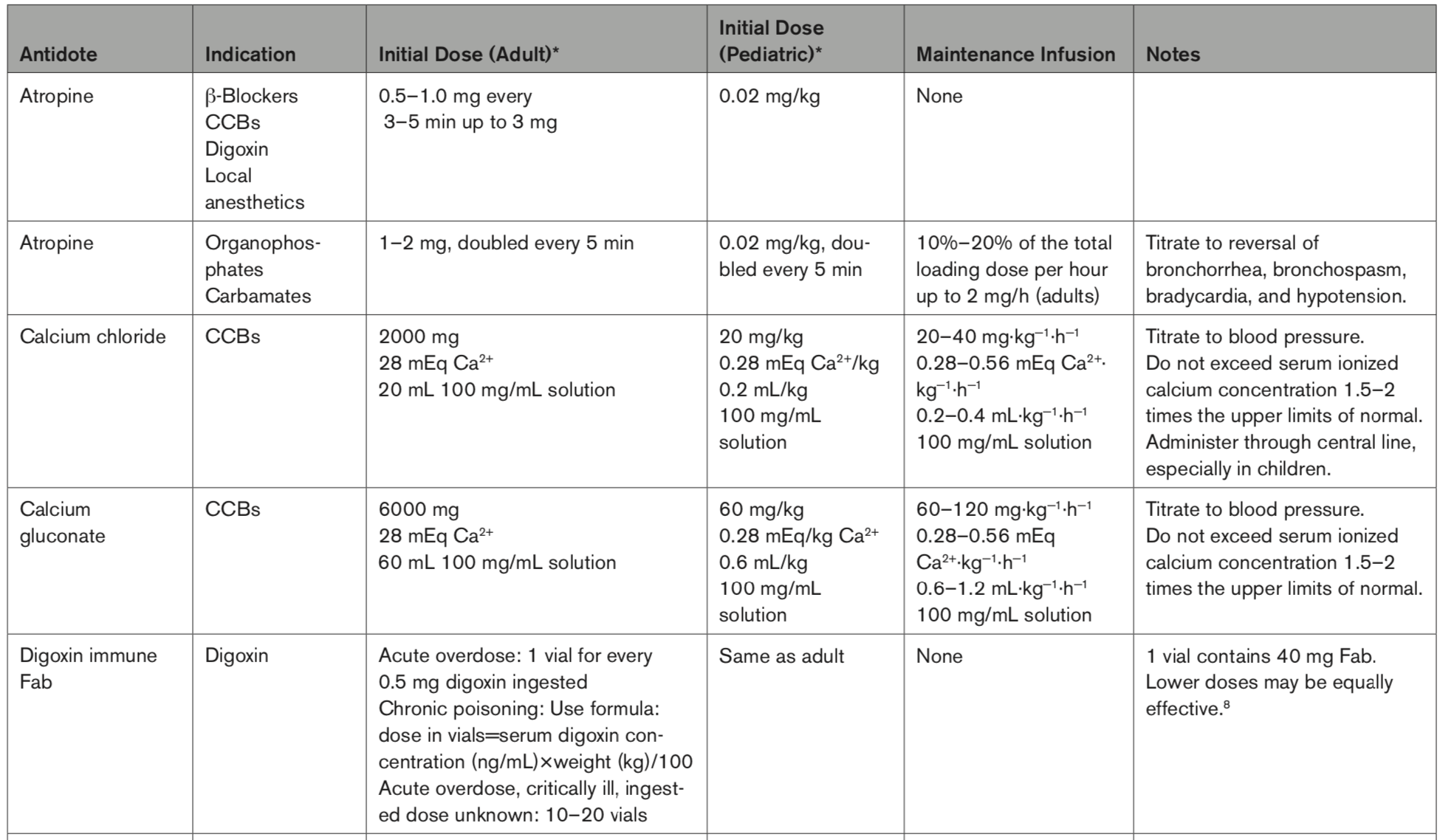
Antidotes

Benzodiazepines
If combined opioid and benzodiazepine poisoning is suspected, it is reasonable to administer nal- oxone first (before other antidotes) for respiratory depression/respiratory arrest. COR 2a, LOE B-NR.
Flumazenil can be effective in select patients with respiratory depression/respiratory arrest caused by pure benzodiazepine poisoning who do not have contraindications to flumazenil. COR 2a, LOE B-NR.
Flumazenil has no role in cardiac arrest related to benzodiazepine poisoning. COR No Benefit, LOE C-EO.
Flumazenil administration is associated with harm in patients who are at increased risk for seizures or dysrhythmias. COR Harm, LOE B-R.
Editorial Comment: Naloxone first, flumazenil only for pure benzo’s (e.g., if used for sedation). Otherwise, avoid flumazenil.
Beta Blockers
We recommend that high-dose insulin be administered for hypotension due to β-blocker poisoning refractory to or in conjunction with vasopressor therapy. COR 1, LOE B-NR.
We recommend that vasopressors be administered for hypotension due to β-blocker poisoning. COR 1, LOE C-LD.
It is reasonable to use a bolus of glucagon, followed by a continuous infusion, for bradycardia or hypotension due to β-blocker poisoning. COR 2a, LOE C-LD.
It is reasonable to utilize extracorporeal life sup- port techniques such as VA-ECMO for life-threatening β-blocker poisoning with cardiogenic shock refractory to pharmacological interventions. COR 2a, LOE C-LD.
It may be reasonable to administer atropine for β-blocker–induced bradycardia. COR 2b, LOE C-LD.
It may be reasonable to attempt electrical pacing for β-blocker–induced bradycardia. COR 2b, LOE C-LD.
It may be reasonable to use hemodialysis for life-threatening atenolol or sotalol poisoning. COR 2b, LOE C-LD.
Intravenous lipid emulsion therapy is not likely to be beneficial for life-threatening β-blocker poisoning. COR Harm, LOE C-LD.
Editorial Comment: Yes to vasopressors and high dose insulin; no to lipid emulsion; consider pacing!
Calcium Channel Blockers
We recommend administering vasopressors for hypotension from calcium channel blocker (CCB) poisoning. COR 1, LOE B-NR.
We recommend administering high-dose insulin for hypotension due to CCB poisoning. COR 1, LOE B-NR.
It is reasonable to administer calcium for CCB poisoning. COR 2a, LOE C-LD.
It is reasonable to administer atropine for hemodynamically significant bradycardia from CCB poisoning. COR 2a, LOE C-LD.
It is reasonable to utilize extracorporeal life support techniques such as VA-ECMO for cardiogenic shock due to CCB poisoning that is refractory to pharma- cological interventions.COR 2a, LOE C-LD.
It might be reasonable to attempt electrical pacing for CCB poisoning with refractory bradycardia. COR 2b, LOE C-LD.
The usefulness of a glucagon bolus and infusion for CCB poisoning is uncertain. COR 2b, LOE C-LD.
The usefulness of administering methylene blue for refractory vasodilatory shock due to CCB poisoning is uncertain. COR 2b, LOE C-LD.
The routine use of intravenous lipid emulsion (ILE) therapy for CCB poisoning is not recommended. COR Harm, LOE C-LD.
Editorial Comment: Yes to vasopressors and high dose insulin; no to lipid emulsion. Try calcium; consider pacing!
Life-Threatening Cocaine Toxicity
We recommend rapid external cooling for life-threatening hyperthermia from cocaine poisoning. COR 1, LOE C-LD.
It is reasonable to administer sodium bicarbonate for wide-complex tachycardia or cardiac arrest from cocaine poisoning. COR 2a, LOE C-LD.
It is reasonable to administer lidocaine for wide-complex tachycardia from cocaine poisoning. COR 2a, LOE C-LD.
It is reasonable to administer vasodilators (eg, nitrates, phentolamine, calcium channel blockers) for patients with cocaine-induced coronary vasospasm or hypertensive emergencies. COR 2a, LOE C-LD.
Editorial Comment: Yes to cooling (preferably immersion), sodium bicarbonate for wide complex tachycardia.
Cyanide
We recommend that hydroxocobalamin be administered for cyanide poisoning. COR 1, LOE C-LD.
We recommend that sodium nitrite be administered for cyanide poisoning when hydroxocobalamin is unavailable. COR 1, LOE C-LD.
In addition to administering hydroxocobalamin or sodium nitrite, it is reasonable to administer sodium thiosulfate for cyanide poisoning. COR 2a, LOE C-LD.
It is reasonable to administer 100% oxygen for cyanide poisoning. COR 2a, LOE C-EO.
Editorial Comment: Yes to hydroxocobalamin. Obtain blood/labs prior to administration. Don’t rely on cyanide levels. Consider cyanide toxicity in those with severely elevated lactate.
Digoxin and Related Cardiac Glycosides
We recommend administration of digoxin-specific antibody fragments (digoxin-Fab) for digoxin or digitoxin poisoning. COR 1, LOE B-NR.
It is reasonable to administer digoxin-Fab for poisoning due to Bufo toad venom and yellow oleander. COR 2a, LOE C-LD.
It may be reasonable to administer digoxin-Fab to treat poisoning from cardiac glycosides other than digoxin, digitoxin, Bufo toad venom, and yellow oleander. COR 2b, LOE C-LD.
It may be reasonable to administer atropine for bradydysrhythmias caused by digoxin and other cardiac glycoside poisoning. COR 2b, LOE C-LD.
It may be reasonable to attempt electrical pacing to treat bradydysrhythmias from digoxin and other cardiac glycoside poisoning. COR 2b, LOE C-LD.
It may be reasonable to administer lidocaine, phenytoin, or bretylium to treat ventricular dysrhythmias caused by digitalis and other cardiac glycoside poisoning until digoxin-Fab can be administered. COR 2b, LOE C-LD.
We do not recommend the use of hemodialysis, hemofiltration, hemoperfusion, or plasmapheresis to treat digoxin poisoning. COR No Benefit, LOE B-NR.
Editorial Comment: Use digoxin specific antibodies; consider pacing!
Local Anesthetic Poisoning
We recommend the administration of intravenous lipid emulsion for local anesthetic poisoning. COR 1, LOE C-LD.
We recommend the use of benzodiazepines to treat seizures associated with local anesthetic systemic toxicity. COR 1, LOE C-LD.
It is reasonable to administer sodium bicarbonate for life-threatening wide-complex tachycardia associated with local anesthetic toxicity. COR 2a, LOE C-LD.
It is reasonable to administer atropine for life- threatening bradycardia associated with local anesthetic systemic toxicity. COR 2a, LOE C-EO
It is reasonable to utilize extracorporeal life support techniques such as VA-ECMO in local anesthetic toxicity with refractory cardiogenic shock. COR 2a, LOE C-EO.
Editorial Comment: Use lipid emulsion; treat seizures with benzo’s; consider bicarb for wide complex tachycardia.
Methemoglobinemia
We recommend administering methylene blue for methemoglobinemia. COR 1, LOE B-NR.
Exchange transfusion may be reasonable as a treatment for methemoglobinemia that is not responsive to methylene blue. COR 2b, LOE C-LD.
Hyperbaric oxygen therapy may be reasonable as a treatment for methemoglobinemia that is not responsive to methylene blue. COR 2b, LOE C-LD.
N-acetylcysteine is not recommended as a treatment for methemoglobinemia. COR No Benefit, LOE B-R.
Ascorbic acid is not recommended as a treatment for methemoglobinemia. COR No Benefit, LOE C-LD.
Editorial Comment: Use methylene blue; consider exchange transfusion or hyperbaric oxygen. No NAC or ascorbic acid.
Opioid Overdose
For patients in respiratory arrest, rescue breathing or bag-mask ventilation should be maintained until spontaneous breathing returns, and standard BLS, ALS, and/or pediatric ALS measures should continue if return of spontaneous breathing does not occur. COR 1, LOE C-LD.
For patients known or suspected to be in cardiac arrest, in the absence of a proven benefit from the use of naloxone, standard resuscitative measures should take priority over naloxone administration, with a focus on high-quality CPR (compressions plus ventilation). COR 1, LOE C-EO.
Lay and trained responders should not delay acti- vating emergency response systems while await- ing the patient’s response to naloxone or other interventions. COR 1, LOE C-EO.
For a patient with suspected opioid overdose who has a definite pulse but no normal breathing or only gasping (ie, a respiratory arrest), in addition to providing standard BLS and/or ALS care, it is reasonable for responders to administer naloxone. COR 2a, LOE B-NR.
Editorial Comment: Use standard BLS/ALS measures, especially if in cardiac arrest. Give naloxone for suspected opioid overdose and respiratory compromise/arrest. Do not give if they have normal respirations but are somnolent.
Opioid Overdose and Successful Response to Naloxone
After return of spontaneous breathing, patients should be observed in a healthcare setting until the risk of recurrent opioid toxicity is low and the patient’s level of consciousness and vital signs have normalized. COR 1, LOE C-LD.
If recurrent opioid toxicity develops, repeated small doses or an infusion of naloxone can be beneficial. COR 2a, LOE C-LD.
Editorial Comment: Monitor closely; if recurrent respiratory depression occurs, give more naloxone.
Organophosphates and Carbamates
We recommend giving atropine immediately for severe poisoning, such as bronchospasm, bronchorrhea, seizures, or significant bradycardia, from organophosphate or carbamate poisoning. COR 1, LOE A
We recommend early endotracheal intubation for life-threatening organophosphate or carbamate poisoning. COR 1, LOE B-NR.
We recommend administration of benzodiazepines to treat seizures and agitation in the setting of organophosphate or carbamate poisoning. COR 1, LOE C-LD.
We recommend use of appropriate personal protective equipment when caring for patients with organophosphate or carbamate exposure. COR 1, LOE C-LD.
We recommend dermal decontamination for external organophosphate or carbamate exposure. COR 1, LOE C-EO.
The use of pralidoxime is reasonable for organophosphate poisoning. COR 2a, LOE A.
Use of neuromuscular blockers metabolized by cholinesterase (ie, succinylcholine and mivacurium) is not recommended for patients with organophosphate or carbamate poisoning. COR No Benefit, LOE C-LD.
Editorial Comment: Give atropine, benzo’s for seizures. Use PPE. Pralidoxime is reasonable. Avoid succinylcholine (use rocuronium) for intubation.
Sodium Channel Blockers
We recommend using sodium bicarbonate to treat life-threatening cardiotoxicity from tricyclic and/or tetracyclic antidepressant poisoning. COR 1, LOE B-NR.
t is reasonable to use sodium bicarbonate to treat life-threatening cardiotoxicity caused by poisoning from sodium channel blockers other than tricyclic or tetracyclic antidepressants. COR 2a, LOE C-LD.
It is reasonable to use extracorporeal life sup- port, such as VA-ECMO, to treat refractory cardiogenic shock from sodium channel blocker poisoning. COR 2a, LOE C-LD.
It may be reasonable to use Vaughan-Williams class Ib antidysrhythmics (eg, lidocaine) to treat life-threatening cardiotoxicity from class Ia or Ic sodium channel blockers. COR 2b, LOE C-LD.
It may be reasonable to use intravenous lipid emulsion to treat life-threatening sodium channel blocker poisoning refractory to other treatment modalities. COR 2b, LOE C-LD.
Editorial Comment: Use sodium bicarb for cardiotoxicity; consider ECMO. May use lidocaine.
Sympathomimetics
We recommend sedation for severe agitation from sympathomimetic poisoning. COR 1, LOE B-NR.
We recommend rapid external cooling for life-threatening hyperthermia from sympathomimetic poisoning. COR 1, LOE C-LD.
Vasodilators, such as phentolamine and/or nitrates, are reasonable for coronary vasospasm from sympathomimetic poisoning. COR 2a, LOE C-EO.
Mechanical circulatory support, such as intra- aortic balloon pump or VA-ECMO, is reasonable for cardiogenic shock from sympathomimetic poisoning refractory to other treatment measures. COR 2a, LOE C-EO.
Prolonged use of physical restraint without sedation is potentially harmful. COR Harm, LOE C-LD.
Editorial Comment: Sedate and cool these patients; consider VA-ECMO; avoid prolonged physical restraints.
ECMO
It is reasonable to use VA-ECMO for persistent cardiogenic shock or cardiac arrest due to poison- ing that is not responsive to maximal treatment measures. COR 2a, LOE C-LD.
It is reasonable to use VA-ECMO for persistent dysrhythmias due to poisoning when other treat- ment measures fail. COR 2a, LOE C-LD.
The effectiveness of VA-ECMO for poisoned patients with cardiovascular collapse from causes other than cardiogenic shock has not been established. COR 2b, LOE C-EO.
Editorial Comment: Consider ECMO in treatment refractory patients.
References:
https://www.ahajournals.org/doi/10.1161/CIR.0000000000001161





1 thought on “2023 AHA Update on Management Cardiac Arrest or Life-Threatening Toxicity Due to Poisoning”
Pingback: LITFL Update 018 • LITFL • Newsletter