
Authors: Genevieve Pentecost, MD (@genpentecost, Emergency Medicine Resident, Washington University School of Medicine in St Louis) and Aaron Lacy, MD (@AaronLacyMD, Assistant Professor of Emergency Medicine, Washington University School of Medicine in St Louis) // Reviewed by: Jamie Santistevan, MD (EM Physician, Presbyterian Hospital, Albuquerque, NM); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Introduction
Welcome back to ECG Pointers from emDOCS. As we all know, a critical concern for emergency physicians is identifying patients with heart tissue-threatening ischemia that could benefit from percutaneous catheterization via stent deployment by an interventional cardiologist. The most common diagnostic test to identify patients who might require percutaneous intervention is the electrocardiogram (ECG). Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention.
ACC/AHA STEMI Diagnostic Criteria [1]
- Men < 40-years-old: ST elevation ≥2.5 mm in V2 or V3, or ≥1 mm in any other leads
- Men ≥40-years-old: ST elevation ≥2 mm in V2 or V3, or ≥1 mm in any other leads
- Women, regardless of age: ST elevation ≥1.5 mm in V2 or V3, or ≥1 mm in any other leads
OMI/NOMI
Over time, the overall sensitivity of the STEMI criteria as an indication for urgent cardiac catheterization has come into question. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG. The chosen vernacular for these ECG findings has been traditionally called “STEMI equivalents”. A major push for a paradigm change from the specialty of emergency medicine has been ongoing, as it is imperative to identify all patients who might benefit from urgent reperfusion therapy.
The paradigm change gained momentum with the introduction of the occlusion myocardial infarction (OMI) versus non-occlusion myocardial infarction (NOMI)[2]. This paradigm shifts seeks to formally recognize signs on the ECG that may represent coronary artery occlusion, and therefore benefit from urgent reperfusion that would otherwise be missed utilizing traditional STEMI criteria. In one study it was found that after cardiac catheterization only 60% of occlusive myocardial infarctions met STEMI criteria[3]. The American College of Cardiology had previously recognized some STEMI equivalents that may benefit from urgent reperfusion therapy, most notably the presence of a new left bundle branch block.
In October 2022, the American College of Cardiology released an updated expert consensus decision regarding the evaluation of chest pain in the emergency department. This included the addition several new STEMI equivalents [4] on ECG that warrant “prompt evaluation for emergency coronary angiography.”
Newest STEMI-equivalents
- Posterior STEMI
- Left bundle branch block with Sgarbossa criteria or Smith-modified Sgarbossa criteria
- Ventricular-paced rhythm with Sgarbossa criteria or Smith-modified Sgarbossa criteria
- De Winter Sign
- Hyperacute T-waves
Example Cases
The following cases represent examples of patients with ECG cases that by the newest STEMI-equivalent consensus decision warrant prompt evaluation for emergency coronary angiography.
Case 1
You are working a busy Monday evening shift and an elderly woman presents with severe chest pressure that began 3 hours ago. She is diaphoretic, pale, and clutching her chest. An ECG is obtained in triage and is shown below. What is the most appropriate next step in management?
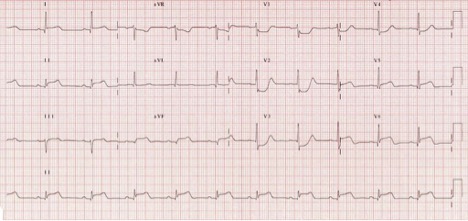
Source: https://litfl.com/posterior-myocardial-infarction-ecg-library/
This case is consistent with a posterior STEMI.
Posterior STEMI [4]
The following ECG features are consistent with the diagnosis of a posterior STEMI
- Horizontal ST-segment depression in V1-V3
- Dominant R-wave (i.e., R-to-S ratio > 1) in V2
- Upright T-waves in anterior leads
- Prominent and broad R-wave (>30 ms)
- Confirmed by ST-segment elevation of 0.5mm in at least 1 of leads V7-V9
A posterior ECG (below) is obtained with V7 at the left posterior axillary line, V8 at the tip of the left scapula, and V9 in the left paraspinal region. Notably, only 0.5mm of elevation is necessary in V7-9 to meet criteria. In addition to a posterior ECG, the ACC’s new recommendations emphasize consideration of an emergent TTE, though lack clarity in defining who should be the operator, stating “a clinician qualified in echocardiography” is necessary, without providing specific definitions.

Source: https://litfl.com/posterior-myocardial-infarction-ecg-library/
You can read more about posterior STEMI in this prior ECG Pointers post: http://www.emdocs.net/ecg-pointers-posterior-mi/#:~:text=Main%20ECG%20pointers%20for%20Posterior,can%20also%20occur%20in%20isolation.
Case 2
An 80-year-old man with a history of 3-vessel CABG, previous VT-arrest s/p pacemaker placement, presents with chest pain for 45 minutes. He is in a paced rhythm on the bedside monitor. An ECG is obtained and is shown below.
Source: https://litfl.com/sgarbossa-criteria-ecg-library/

This case is consistent with the Smith-modified Sgarbossa Criteria.
Smith-modified Sgarbossa criteria [4,5]
Notably in the newest ACC guidelines, a new LBBB alone is no longer considered a STEMI equivalent. However, it still serves as evidence of a patient’s elevated risk for underlying coronary artery disease or cardiomyopathy. There are multiple criteria systems for diagnostic an acute myocardial infarction in this population, as well as patients with ventricular-paced rhythms. The ACC endorses the use of the Smith-modified Sgarbossa criteria, which is applicable to patients with a left bundle branch block or a ventricular-paced rhythm. The presence of any of the following is considered a STEMI-equivalent.
- Concordant ST-segment elevation of ≥ 1 mm in leads with a positive QRS complex
- Concordant ST-segment depression of ≥ 1 mm in V1-V3
- ST-segment elevation at the J-point, relative to the QRS onset, is at leads 1 mm and has an amplitude of at least 25% of the preceding S-wave
Case 3
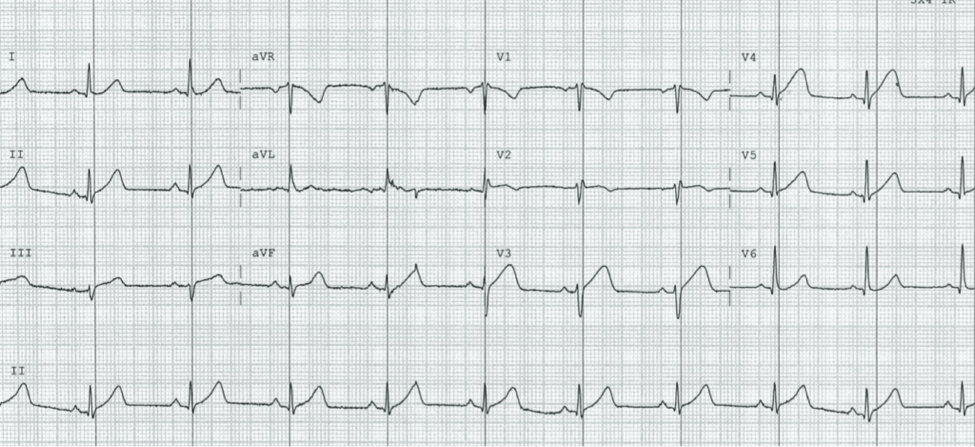
A 71-year-old woman presents with dyspnea, lightheadedness, and pre-syncope for 2 hours. Her vital signs are stable. Her ECG is shown below.

Source: https://litfl.com/de-winter-t-wave/
This case is consistent with the De Winter Sign.
De Winter Sign [4,6]
First described in 2008 this pattern be seen in proximal left anterior descending artery occlusion and should be evaluated by emergent angiography. Features of De Winter sign include:
- Tall, prominent, symmetrical T-waves that arise from an upsloping ST-segment depression > 1 mm at the J-point in precordial leads
- 5-1 mm ST-segment elevation in aVR
Case 4
A middle-aged male presents to your emergency department after waking up with pressure like chest pain that radiates to his jaw. He informs you he has a history of hypertension, hyperlipidemia, and smokes daily. He underwent serial ECGs, which are shown below.
Time 0 ECG:

Source: https://litfl.com/ecg-case-125/
Time +15 minutes ECG:
Source: https://litfl.com/ecg-case-125/
Time +30 minutes ECG:

Source: https://litfl.com/ecg-case-125/
These ECGs are consistent with hyperacute T-waves that evolve into STEMI.
Hyperacute T-waves
Features of hyperacute T waves include:
- Morphology can be variable, but includes broad, asymmetric, peaked T-waves. This may indicate evidence of early coronary arteryocclusion
- More consistently you will see T-waves that are large relative the QRS and often the R wave amplitude is reduced
- Serial ECGs over very short intervals should be used to judge progression to STEMI
Wrap-Up
In addition to defining these STEMI equivalents, the updated 2022 ACC recommendations provide commentary regarding evaluation of patient by 3 groupings: 1) STEMI or STEMI-equivalents, 2) ischemic ECG findings, and 3) non-ischemic ECG findings. This includes pathways specific for ECG patterns concerning for acute or subacute subendocardial myocardial ischemia (e.g., aVR ST-segment elevation, ST-segment depression, Wellen’s syndrome, and T-wave inversions). Specifically, the ACC recommends these be treated as NSTEMI-equivalents unless additional clinical findings warrant more urgent or emergent coronary angiography. They also redefine the terminology used to describe chest pain, phasing out the use of “typical” and “atypical” chest pain, while emphasizing the terms “cardiac, possible cardiac, and noncardiac” to describe chest pain. In all, this 2022 update from the ACC provides diagnosis and management pathways intended to guide the approach to chest pain in the emergency department.
Main ECG Pointers:
- Many patients that would benefit from PCI may not meet traditional STEMI criteria on their ECG.
- The current STEMI vs NSTEMI paradigm may prevent some NSTEMI patients from receiving emergent reperfusion despite the presence of coronary artery occlusion.
- The nomenclature Occlusive Myocardial Infarction (OMI) and Non-occlusive myocardial infarction (NOMI) may better encompass those that would benefit from PCI.
- STEMI-equivalent findings on an ECG that are indicative of coronary artery occlusion include: posterior STEMI, De Winter Sign, Smith-modified Sgarbossa criteria and hyperacute T Waves.
References
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). J Am Coll Cardiol. 2018 Oct 30;72(18):2231-2264.
- P. Meyers, S.D. Weingart, S.W. Smith. The OMI manifesto. Dr. Smith’s ECG Blog. Available: http://hqmeded-ecg.blogspot.com/2018/04/the-omi-manifesto.html (2018)
- Meyers HP, Bracey A, Lee D, Lichtenheld A, Li WJ, Singer DD, Kane JA, Dodd KW, Meyers KE, Thode HC, Shroff GR, Singer AJ, Smith SW. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. J Emerg Med. 2021 Mar;60(3):273-284.
- Writing Committee; Kontos MC, de Lemos JA, Deitelzweig SB, Diercks DB, Gore MO, Hess EP, McCarthy CP, McCord JK, Musey PI Jr, Villines TC, Wright LJ. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2022 Nov 15;80(20):1925-1960. PMID: 36241466.
- Smith SW, Dodd KW, Henry TD, Dvorak DM, Pearce LA. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med. 2012 Dec;60(6):766-76.
- de Winter RJ, Verouden NJ, Wellens HJ, Wilde AA; Interventional Cardiology Group of the Academic Medical Center. A new ECG sign of proximal LAD occlusion. N Engl J Med. 2008 Nov 6;359(19):2071—2073. PMID: 18987380.





1 thought on “ECG Pointers: STEMI Equivalents from the American College of Cardiology”
Pingback: STEMI/NSTEMI vs. OMI/NOMI and STEMI equivalents - KINNETIC MEDICINE