
Author: Rachel Bridwell, MD (@rebridwell, EM Resident Physician, San Antonio, TX) // Edited by: Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) and Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital)
Welcome to EM@3AM, an emDocs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 62-year-old male is brought in by EMS for altered mental status and complaints of visual disturbances. Per EMS report, the patient had a homemade moonshine still in his living room. The patient is confused though complains that his vision is globally diminished as if he were looking through a snowstorm. Review of systems is remarkable for a headache and dizziness.
Triage vital signs (VS): BP 105/50, HR 122, T 99.9 Oral, RR 35, SpO2 96% on room air.
Exam:
Alert and oriented to self and place only; confused.
Neurological: Cranial nerves II-XII intact. Deep tendon reflexes (triceps, biceps, patellar) 2+ bilaterally. Muscle strength 5/5 upper and lower extremity large muscle groups. Two-point discrimination intact distally in all extremities. Ataxic gait. HEENT: Moderately poor dentition, oral cavity smells of solvent, EOMI, Pupils 5 mm bilaterally and poorly reactive. VA: 20/230 despite corrective lenses. Fundoscopic exam reveals hyperemic optic nerves bilaterally. CV: Tachycardic, but no murmurs, rubs, or gallops. Pulmonary: Tachypneic, lungs clear to auscultation bilaterally. Abdomen: soft, mildly and diffusely tender. Integumentary: Without rashes, lesions, excoriations, or tract marks. EKG: Heart rate 110 beats per minute, but otherwise normal.
What’s the diagnosis, and what’s your next step in your evaluation and treatment?
Answer: Methanol Poisoning1-8
- Epidemiology:
- Accidental ingestions from windshield wiper fluid or car cleaning solvent.
- Intentional ingestions are due to those who confuse it for ethanol or cannot afford ethanol.
- Outbreaks of tainted beverages occur worldwide, with 1000 patient exposed in Libya in 2013; case fatality rate of 10%.2
- Can be absorbed though skin or inhalation, though rarely causes systemic toxicity.
- Background: methanol => formaldehyde => formic acid => (req folate) => CO2+ H2O
- Formic acid toxic metabolite by inhibiting oxidative phosphorylation.
- Pharmacology: Absorption 30-60 min, metabolism 8.5 mg/dL/hr, minimum lethal dose 1g/kg or 100 cc in an adult.
- Clinical Presentation:
- Early—HA, dizziness, vertigo, “snow field” vision, mild inebriation.
- Late—Tachycardia, hypotension, tachypnea (compensation for metabolic acidosis), abdominal pain as osmolar gap and acidosis increases. Severe cases can precipitate rhabdomyolysis and renal failure.3
- Evaluation:
- Assess ABCs and obtain VS.
- Dependent on amount ingested and coingestion of other alcohols; mental status and vitals vary.
- Perform a complete physical examination. The following findings are associated with methanol ingestion, evolving over 6-24 hours but can extend to 96 hours.4
- HEENT: VA bilaterally diminished, hyperemic optic discs, IOP normal.
- Cardiovascular: Tachycardia.
- Pulm: Tachypneic with clear lungs => Metabolic Acidosis.
- Abdomen: Diffusely tender => Methanol is a GI irritant.
- Laboratory evaluation:
- CBC, BMP, VBG with lactate, serum ketones, LAEs—blood glucose >140 is a poor prognostic risk factor for mortality.5
- Methanol level, ASA, salicylates in setting of coingestion, and VBG (anion gap metabolic acidosis, or AGMA).
- Osmolar Gap: Calculated Osm – Actual Osm
- Serum Osmolarity = 2*Na+ BUN/2.8 + glucose/18+ethanol/4.6 + isopropanol/6.0 + methanol/3.2 + ethylene glycol/6.2
- Imaging: NCHCT for workup of AMS; MRI may show bilateral putamen necrosis and subcortical white matter damage.6
- Treatment:
- Gastric decontamination not useful to due rapid absorption.
- Fluid resuscitation and treat metabolic acidosis.
- Fomepizole: 15 mg/kg loading dose, 10 mg/kg q12hr x 4 doses, 15 mg/kg q12hr.
- If fomepizole unavailable or contraindicated (i.e. known allergy), use ethanol PO or IV to inhibit alcohol dehydrogenase.
- Target serum level 100-150 mg/dL—100 mg/kg IV (requires central line).
- Austere environment: 3-4 1 oz. shots of 80 proof alcohol for loading dose with maintenance dose of 1-2 shots/hr for 70 kg human.7
- Risk is hyperglycemia.
- Bicarb—Infusions to maintain pH>7.30.7
- Hemodialysis (HD>CRRT)
- Refractory metabolic acidosis
- Visual abnormalities
- Renal insufficiency
- Hemodynamic deterioration in spite of aggressive resuscitation
- Electrolyte derangements refractory to persistent correction
- Vitamin therapy
- Folinic acid (leucovorin) or folic acid 1 mg/kg (max 50 mg) q4-6 hours required for breakdown of formic acid.8
- Disposition:
- Consult medical toxicologist and local poison control center.
- ICU admission for serious signs and symptoms of methanol ingestion.
- Transfer to facility with hemodialysis available.
- Observe 12 hours and discharge home if: discussed with toxicology/poison center and patient is asymptomatic, no osmolar gap, no metabolic acidosis, and no anion gap.
- Pearls:
- Acidemia is greatest predictor of final visual acuity.9
- Dose to cause permanent visual impairment is approximately 30cc, or a mouthful.
- Delayed Parkinsonism and polyneuropathy can occur later.
- John Milton, author of Paradise Lost, went blind from methanol poisoning.
From Dr. Katy Hanson at Hanson’s Anatomy:


Which of the following laboratory findings suggests ethylene glycol ingestion?
A) Anion gap 16 and pH 7.32 associated with vision changes
B) Lactate 0.9 mmol/L, pH 7.12, and creatinine 2.5 mg/dL
C) Osmol gap 20, anion gap 8, and ketonemia
D) pH 7.10, lactic acid 5.5 mmol/L, and anion gap 21
Answer: B
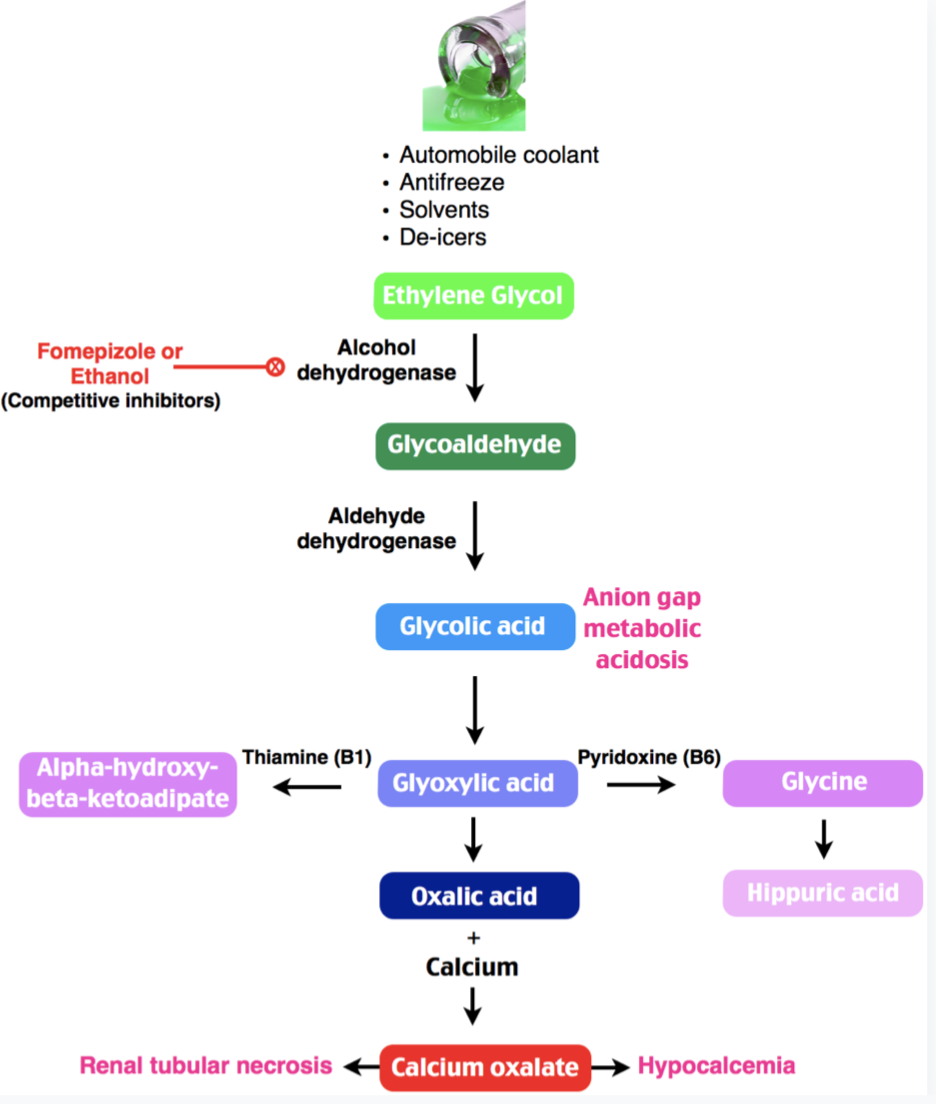
The toxic alcohols include ethanol, ethylene glycol, methanol, and isopropanol. Each alcoholic overdose has its own clinical characteristic. Markers of intoxication with ethylene glycol include high anion gap metabolic acidosis with an absence of significant lactate or ketone concentrations, calcium oxalate formation leading to acute renal failure. Therefore, lactate 0.9 mmol/L, pH 7.12, and creatinine 2.5 mg/dL would be characteristic of ethylene glycol poisoning; although, lactate can be slightly elevated (both falsely or truly), but not at levels that would explain the the significant acidosis. Sodium bicarbonate may be used for urine alkalinization to improve acidemia. Ethanol or fomepizole may be utilized for acute management in conjunction with a nephrology consultation. Hemodialysis is indicated for ethylene glycol levels > 25 mg/dL. Adjunctive therapy includes thiamine and pyridoxine every 4 to 6 hours.
Anion gap 16 and pH 7.32 (A) associated with vision changes characterizes acute methanol toxicity. This leads to high anion gap metabolic acidosis with “snow field” vision, blindness, or optic disc hyperemia or retinal edema on fundoscopy. Osmol gap 20, anion gap 8, and ketonemia (C) suggests acute isopropanol (isopropyl alcohol) poisoning, which leads to ketosis without acidosis, a normal anion gap, and an elevated osmol gap. A pH of 7.10, lactic acid 5.5 mmol/L, and anion gap 21 (D) is nonspecific and may represent metabolic acidosis from sources other than toxic ingestions, such as sepsis.
FOAMed:
https://emergencymedicinecases.com/toxic-alcohols/
http://www.emdocs.net/the-unhappy-drunk-toxic-alcohols/
https://lifeinthefastlane.com/toxic-alcohol-ingestion/
http://foamcast.org/2016/02/18/episode-43-alcohols/
http://www.emdocs.net/toxcard-toxic-alcohol-poisoning/
https://coreem.net/podcast/episode-129-0-toxic-alcohols/
References:
- Kraut JA, Mullins ME. Toxic Alcohols. N Engl J Med 2018; 378:270-280.
- Rostrup M, Edwards JK, Abukalish M, Ezzabi M, Some D. (2016): The Methanol Poisoning Outbreaks in Libya 2013 and Kenya 2014. PLOS ONE 11(6):e0157256.
- Grufferman S, Morris D, Alvarez J: Methanol poisoning complicated by myoglobinuric renal failure. Am J Emerg Med 3: 24, 1985.
- Haviv YS, Rubinger D, Zamir E, Safadi R. Pseudo-normal osmolal and anion gaps following simultaneous ethanol and methanol ingestions. Am J Nethprol. 1998; 18:436-438.
- Sanaei-Zadeh H, Esfeh SK, Zamani N, Jamshid, F, Shadnia S. Hyperglycemia is a Strong Prognostic Factor of Lethality in Methanol Poisoning. J Med Toxicol. 2011; 7(3): 189-194.
- Jain N, Himanshu D, Verma SP, Parihar A: Methanol poisoning: characteristic MRI findings. Ann Saudi Med 33: 68, 2013.
- Li J, Mills T, Erato R: Intravenous saline has no effect on blood ethanol clearance. J Emerg Med 17: 1, 1999.
- Barceloux DG, Bond GR, Krenzelok EP, et al: American Academy of Clinical Toxicology Ad Hoc Committee on the Treatment Guidelines for Methanol Poisoning: American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol 40: 415, 2002
- Desai, T, Sudahlkar, A, Vyas, U. Methanol Poisoning: Predictors of Visual Outcomes. JAMA Ophthalmol. 2013;131(3):358-364.




