Authors: Katey DG Osborne, MD (EM Attending Physician; Tacoma, WA), Rachel Bridwell, MD (EM Attending Physician; Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX)
Welcome to emDOCs revamp! This series provides evidence-based updates to previous posts so you can stay current with what you need to know.
A 55-year-old male, with a previous medical history of hypertension, hyperlipidemia, and gout, presents to the emergency department for four days of fever and progressive rash. He denies recent travel or exposure to new skin products, laundry detergents, or pets. His PCP started him on allopurinol 4 weeks ago after his first gout flare.
Triage vital signs (VS): BP 140/80 mm Hg, HR 112 BPM, T 102.1F, RR 14 bpm, SpO2 99% on room air.
Pertinent physical examination findings:
HEENT: Periorbital edema, oropharynx without erythema or edema.
Neck: Presence of anterior and posterior chain cervical lymphadenopathy.
Cardiovascular: Tachycardic, regular rhythm.
Lungs: Clear to auscultation bilaterally.
Skin: Blanchable morbilliform rash localized to the face, upper extremities, and trunk.
What is the next step in your evaluation and treatment?
Answer: Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Syndrome1-5
Definition / Clinical Presentation:
- Also known as Drug-Induced Hypersensitivity Syndrome
- Defined as a particular drug reaction occurring in the first 2 months after drug initiation characterized by morbilliform cutaneous eruption with fever, malaise, facial edema, lymphadenopathy. 1,2
- The presenting symptoms in almost all patients are skin rash, liver involvement, hypereosinophilia, and lymphadenopathy.
- Consideration of the diagnosis regardless of skin eruption in patients with hypereosinophilia, liver involvement, fever, and lymphadenopathy.3
- DRESS syndrome can have systemic involvement to include: 2
- Acute hepatitis (most common)
- Interstitial nephritis
- Interstitial pneumonitis
- Myocarditis – hypersensitivity or acute necrotizing eosinophilic myocarditis (ANEM)
- While majority cases are mild to moderate, severe DRESS can present with acute renal failure, acute respiratory distress syndrome (ARDS), liver failure, and sepsis.2
- DRESS Syndrome has a 10% mortality rate with the primary cause of mortality being hepatic necrosis.2
Etiology: 1,2,4
- Drugs most implicated in the etiology of DRESS:
- Aromatic Anti-epileptic Drugs: carbamazepine (most common), phenytoin, phenobarbital, lamotrigine
- Allopurinol (2nd most common)
- Sulfonamides: Trimethoprim- Sulfamethoxazole (TMP-SMX), dapsone, sulfasalazine
- Minocycline
- Vancomycin
- Pathogenesis not fully understood:
- Theorized predominantly due to genetic mutations in drug detoxification enzymes leading to accumulation of toxic metabolites.
- Drug is identified as the inciting agent in 80% of cases.
- Human Herpesviridae (HHV-6, HHV-7 CMV, or EBV) infection / reactivation may be a risk factor.
- Suspect a small subset due to delayed T-cell mediated hypersensitivity reaction.
- Theorized predominantly due to genetic mutations in drug detoxification enzymes leading to accumulation of toxic metabolites.
Risk Factors:
- Previous history of a drug reaction
- A family history of DRESS in a primary relative
Evaluation:
- Assess ABCs and obtain vital signs:
- Fever occurs in majority of patients3
- Tachypnea, hypoxia, and/or hypotension can be indicative of cardiac or pulmonary involvement.
- Altered mentation / encephalopathy can be concerning for hepatic failure.
- Perform a thorough history:
- Query specifically about new medications, drug allergies, and family history of DRESS.
- Perform a physical exam:
- Skin Lesions – Rash occurs in nearly 99% of patients.2,4
- Early: symmetric morbilliform eruption (picture 1) on the face, upper trunk and extremities; indistinguishable from an exanthematous drug eruption
- Late: If drug is not discontinued, the eruption can progress to generalized exfoliative dermatitis with associated sterile bullae, and lower extremity purpura.
- Skin Lesions – Rash occurs in nearly 99% of patients.2,4

Picture 1: Symmetric morbilliform eruption of the trunk 5
- Facial Edema
- Mucous Membranes: pharyngitis / tonsillar edema, cheilitis, mucosal erosions2
- Hepatomegaly
- Diffuse lymphadenopathy
- Laboratory evaluation:
- CBC with differential
- Eosinophilia (30% of cases)1
- Atypical lymphocytes
- Basic Metabolic Panel
- Liver Function Tests:
- Elevated ALT (seen in 70% of cases), AST, and alkaline phosphatase2,3
- Renal function panel and urinalysis (UA) with microscopy2
- May show elevated serum creatinine.
- UA with mild hematuria, proteinuria, and eosinophils – indicative of nephritis
- PT/INR & PTT – if evidence of hepatic involvement
- Cardiac enzymes – if patient has chest pain or other anginal equivalents
- Consideration of viral hepatitis panel and serology.
- Rule out confounding viral or autoimmune hepatitis.
- ESR & CRP – nonspecific and typically elevated
- Blood culture – if presenting with sepsis
- CBC with differential
- Imaging:
- Consider a chest radiograph in patients with pulmonary symptoms to evaluate for associated pneumonitis, pleural effusions, cardiomegaly.
- Obtain EKG if patient is presenting with chest pain.
Diagnosis:
- No reliable standard for diagnosis
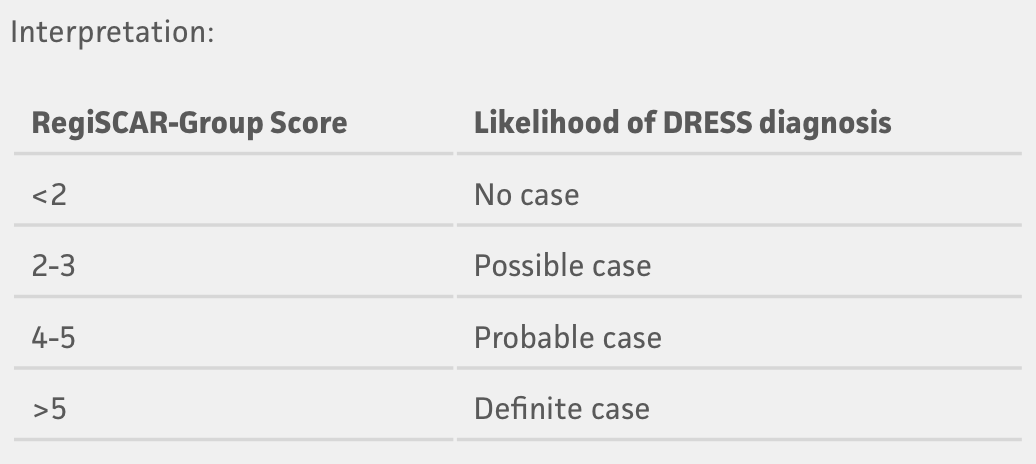
- RegiSCAR Criteria identifies vast majority of cases retrospectively 3,4
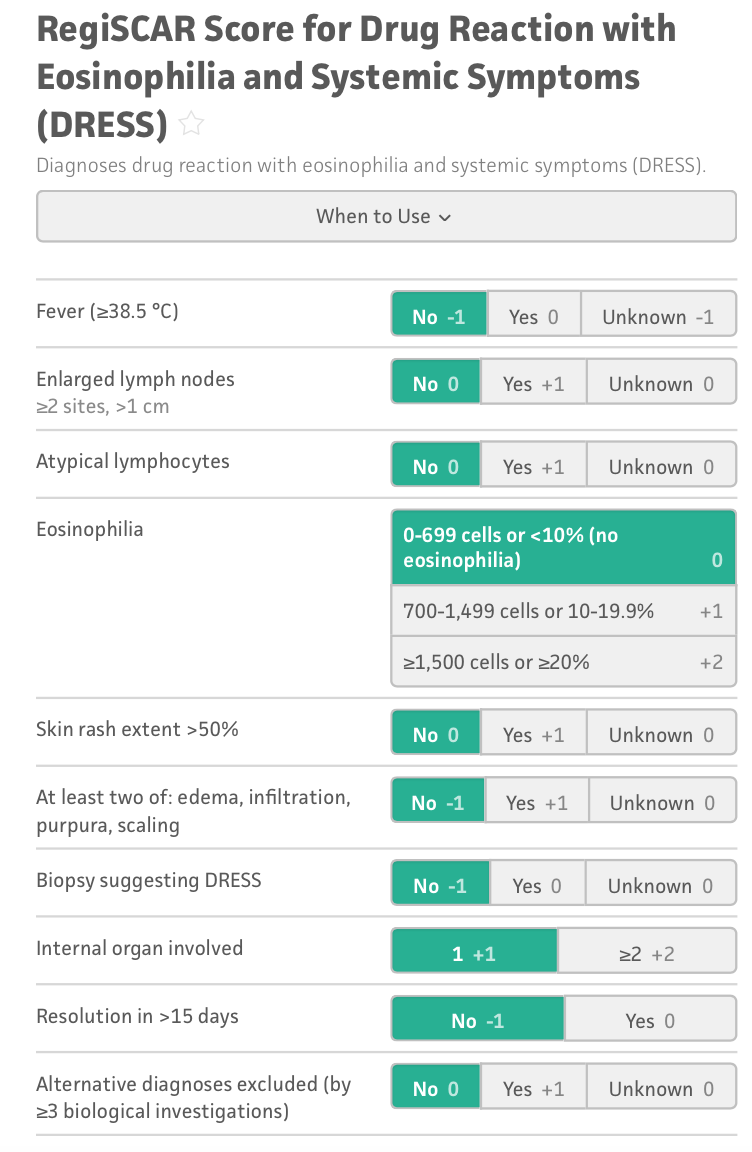
*Rash suggestive of DRESS requires 2 of the following: Purpuric lesions (other than legs), infiltration, facial edema, or psoriasiform desquamation.
Treatment:
- Identify the offending agent and discontinue.
- DRESS syndrome eruption will remain present for weeks to months following discontinuation of the inciting agent.6
- Initiate systemic steroid therapy with 1 mg/kg/day prednisone when diagnosis is considered.
- Systemic therapy may result in improvement of symptoms and labs, but may not prevent progression to or management of end-organ dysfunction.7
- Recurrence of rash and hepatitis may occur with rapid discontinuation of systemic steroids – they should be tapered over 3 – 6 months.1,4
- Avoid empiric antibiotics as cross reactivity can aggravate presentation.
- Progression of systemic disease despite steroid administration can be managed with the addition of IVIG and consideration of plasmapheresis, immunosuppressive agents (cyclophosphamide, cyclosporin, etc.), and/or N-acetylcysteine (NAC). 4,7
Disposition:
- Admission with Dermatology consultation
- Critical Care involvement for severe DRESS syndrome in cases of hepatic and/or renal failure.
- Burn center transfer for management of severe exfoliative dermatitis
- Predictive factors for serious cases have yet to be identified, however allopurinol associated DRESS has a higher associated progression to serious DRESS and death rate.3
- Patients should be made aware of their specific drug hypersensitivity and these drugs should never be readministered as clinical findings recur more rapidly and with increased severity.1,2
Pearls:
- Allopurinol and carbamazepine are the most implicated drugs, however, over 50 drugs as well as viruses have been shown to precipitate DRESS syndrome.
- Differentiated from other diagnoses due to characteristic latent period of 2-6 weeks from onset of drug initiation.
- The most common visceral organ involvement is the liver with hepatomegaly or transaminase elevation.
- DRESS syndrome has a 10% mortality rate.
Further Reading:
- emdocs.net DRESS: what does the emergency physician need to know?
- First 10 in EM DRESS syndrome– a rapid review
References:
- Saavedra AP, Roh EK, Mikailov A. Adverse Cutaneous Drug Reactions. In: Fitzpatrick’s Color Atlas and Synopsis of Clinical Dermatology. 9th ed. McGraw-Hill Education; 2023.
- Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: Part I. Clinical perspectives. J Am Acad Dermatol. 2013;68(5):693.e1-693.e14.
- Cacoub P, Musette P, Descamps V, et al. The DRESS Syndrome: A Literature Review. Am J Med. 2011;124(7):588-597.
- Gottlieb M, Figlewicz MR, Rabah W, Buddan D, Long B. Drug reaction with eosinophilia and systemic symptoms: An emergency medicine focused review. Am J Emerg Med. 2022;56:1-6.
- Kocaoglu C, Cilasun C, Solak ES, Kurtipek GS, Arslan S. Successful Treatment of Antiepileptic Drug-Induced DRESS Syndrome with Pulse Methylprednisolone. Case Rep Pediatr. 2013;2013:928910.
- Tetart F, Picard D, Janela B, Joly P, Musette P. Prolonged Evolution of Drug Reaction With Eosinophilia and Systemic Symptoms: Clinical, Virologic, and Biological Features. JAMA Dermatol. 2014;150(2):206-207.
- Husain Z, Reddy BY, Schwartz RA. DRESS syndrome: Part II. Management and therapeutics. J Am Acad Dermatol. 2013;68(5):709.e1-709.e9.




