Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK)

The American College of Gastroenterology recently released updated guidelines for managing patients with lower GI bleeding (LGIB). This post will provide the major takeaways for emergency clinicians.
Background
Acute LGIB results in over 100,000 admissions in the U.S. annually, and the incidence appears to be increasing based on current literature.
There are a significant number of etiologies for LGIB. Diverticulosis is the most common cause, though this varies based on the population. Other causes include ischemic colitis, hemorrhoids, angioectasias, colorectal neoplasia, postpolypectomy bleeding, colitis (inflammatory, infectious, or radiation-related), rectal/stercoral/NSAID-induced ulcers, and radiation proctopathy.
Significant risk factors for LGIB include antiplatelet use such as aspirin, NSAIDs, and P2Y12 inhibitors like clopidogrel, older age, and diverticulosis.
Recommendation Grading and Strength
Strong recommendation: evidence shows the benefit of the intervention or treatment clearly outweighs any risk.
Conditional recommendation: there is uncertainty as to the risk:benefit ratio.
High certainty of evidence: further research is unlikely to change the confidence in the estimate of the effect.
Moderate certainty of evidence: further research is likely to have an important impact and may change the estimate.
Low certainty of evidence: further research is very likely to change the estimate.
Initial triage/evaluation
Key Concept: A focused history, physical examination, and laboratory evaluation should be obtained at the time of patient presentation to assess the severity of bleeding and its possible location and etiology. Initial patient assessment and hemodynamic resuscitation should be performed simultaneously.
Risk assessment
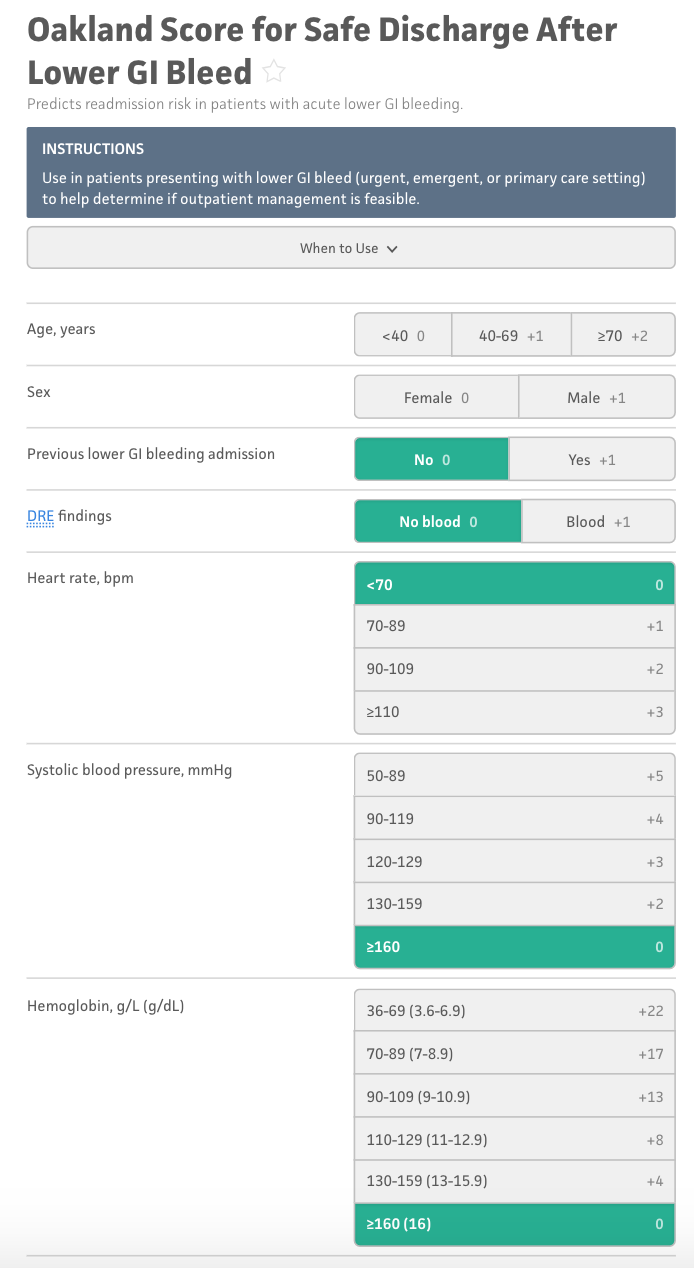
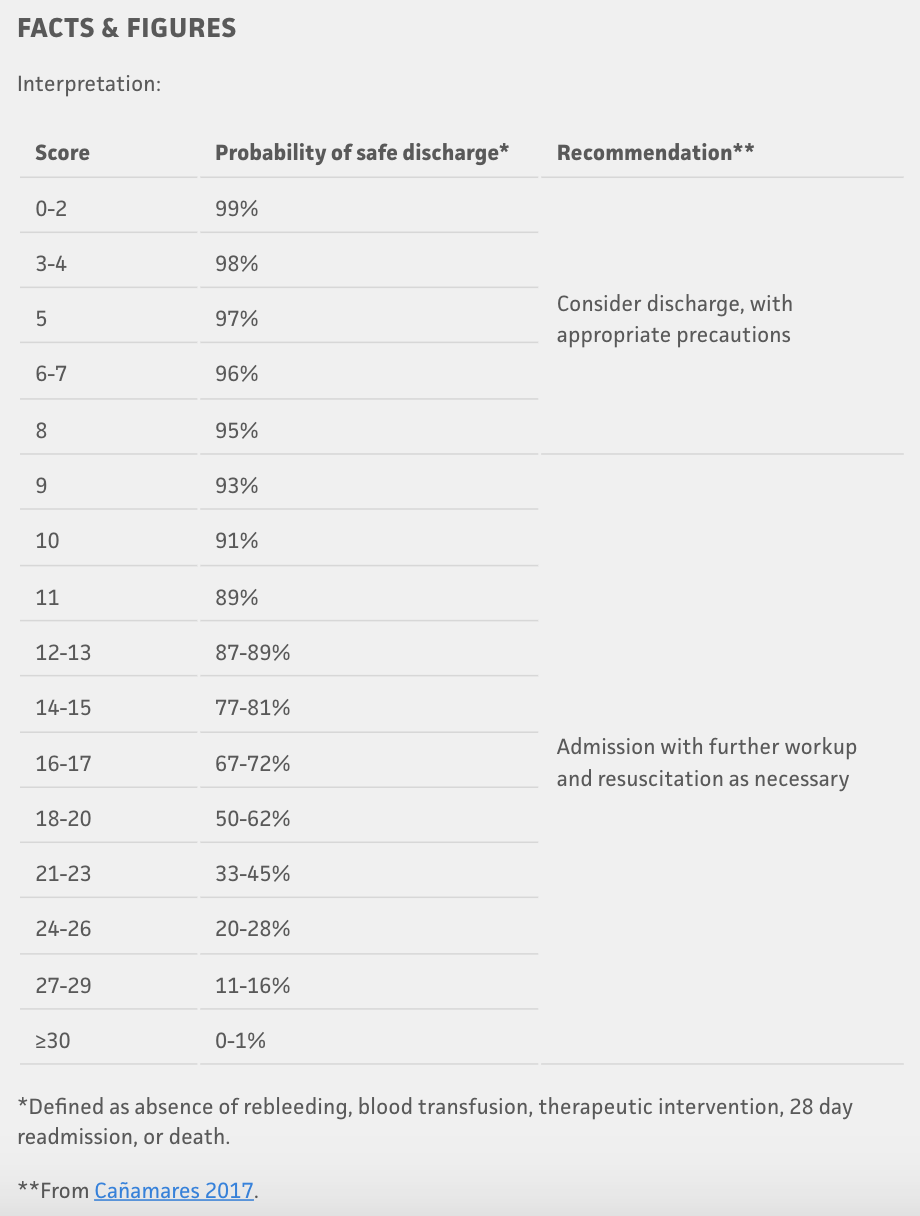
Recommendation: We suggest using risk stratification tools (e.g., Oakland score #8) to identify low-risk patients with LGIB who are appropriate for early discharge and outpatient diagnostic evaluation. Risk scores should be used to supplement but not replace clinician judgment. (Conditional recommendation, low-quality evidence).
Hemodynamic resuscitation
Key Concept: Patients with hemodynamic instability and/or suspected ongoing bleeding should receive intravenous fluid resuscitation with the goal of optimization of blood pressure and heart rate before endoscopic evaluation/intervention.
Recommendation: We suggest a restrictive strategy of red blood cell transfusion (threshold for transfusion at a hemoglobin level of 7 g/dL) in hemodynamically stable patients with LGIB. (Conditional recommendation, low-quality evidence).
Exclusion of proximal source of bleeding
Key Concept: Hematochezia associated with hemodynamic instability may be indicative of an UGIB source, and an upper endoscopy should be performed if the suspicion is high to exclude a proximal source of bleeding.
Management of patients on VKAs
Key Concept: Endoscopic hemostasis can be considered safe and effective in patients who have an international normalized ratio (INR) of 2.5 or less.
Recommendation: Although most patients with LGIB on VKAs are unlikely to require reversal, we suggest reversal of patients who present with a lifethreatening LGIB and have an INR substantially exceeding the therapeutic range. For patients on VKAs to prevent stroke in nonvalvular atrial fibrillation who require reversal, 4-factor prothrombin complex concentrate (PCC) is preferred to fresh frozen plasma (FFP) because of the rapidity of INR reduction (Conditional recommendation, very low-quality evidence).
DOAC reversal
Recommendation: For patients on DOACs, we suggest reversal for the small subset of patients who present with a life-threatening LGIB that does not respond to initial resuscitation and cessation of the anticoagulant alone. For patients requiring reversal, targeted reversal agents (idarucizumab for dabigatran and andexanet alfa for apixaban and rivaroxaban) should be used when available if the DOAC has been taken within the past 24 hours (Conditional recommendation, very low-quality evidence).
Management of antiplatelets in an acute setting
Key Concept: Platelets should be administered in the setting of severe LGIB to maintain a platelet count of .30 3 109 /L, and a higher threshold of .50 3 109 /L can be considered if endoscopic procedures are required. There is no benefit to routine platelet transfusion for patients on antiplatelets.
Key Concept: For patients with LGIB on cardiac aspirin for secondary prevention, aspirin should be continued during hospitalization if possible. Nonaspirin antiplatelets should be held initially for patients with severe hematochezia. However, for patients with recent cardiac stents within 1 year, a multidisciplinary approach should be used to determine the safety of temporarily holding antiplatelets.
Role of antifibrinolytic agents
Recommendation: We recommend against the administration of antifibrinolytic agents such as tranexamic acid in LGIB. (Strong recommendation, moderate quality evidence).
Role of colonoscopy
Key Concept: The colonic mucosa should be carefully inspected during insertion and withdrawal, with aggressive attempts to wash residual stool and blood to identify bleeding sites. The terminal ileum should be intubated to exclude proximal sources of bleeding when feasible if a colonic source of bleeding is not found. The use of a clear cap is recommended to assist in detection and treatment of bleeding.
Recommendation: We recommend the performance of colonoscopy for most patients who are hospitalized with LGIB because of its value in detecting a source of bleeding (Strong recommendation, lowquality evidence).
Recommendation: However, colonoscopy may not be needed in patients where bleeding has subsided, and the patient has had a high-quality colonoscopy within 12 months with an adequate bowel preparation showing diverticulosis with no colorectal neoplasia. (Conditional recommendation, very low-quality evidence).
Role of CTA
Recommendation: We suggest performing a CTA as the initial diagnostic test in patients with ongoing hemodynamically significant hematochezia. However, CTA is of low yield in patients with minor LGIB or those in whom bleeding has clinically subsided. (Conditional recommendation, low-quality evidence).
Management of Positive CTA
Recommendation: We recommend that patients who have a CTA demonstrating extravasation be promptly referred to interventional radiology for transcatheter arteriography and possible embolization. For specialized centers with experience in performing endoscopic hemostasis, a colonoscopy can also be considered after a positive CTA. (Strong recommendation, moderate quality evidence).
Timing of Colonoscopy
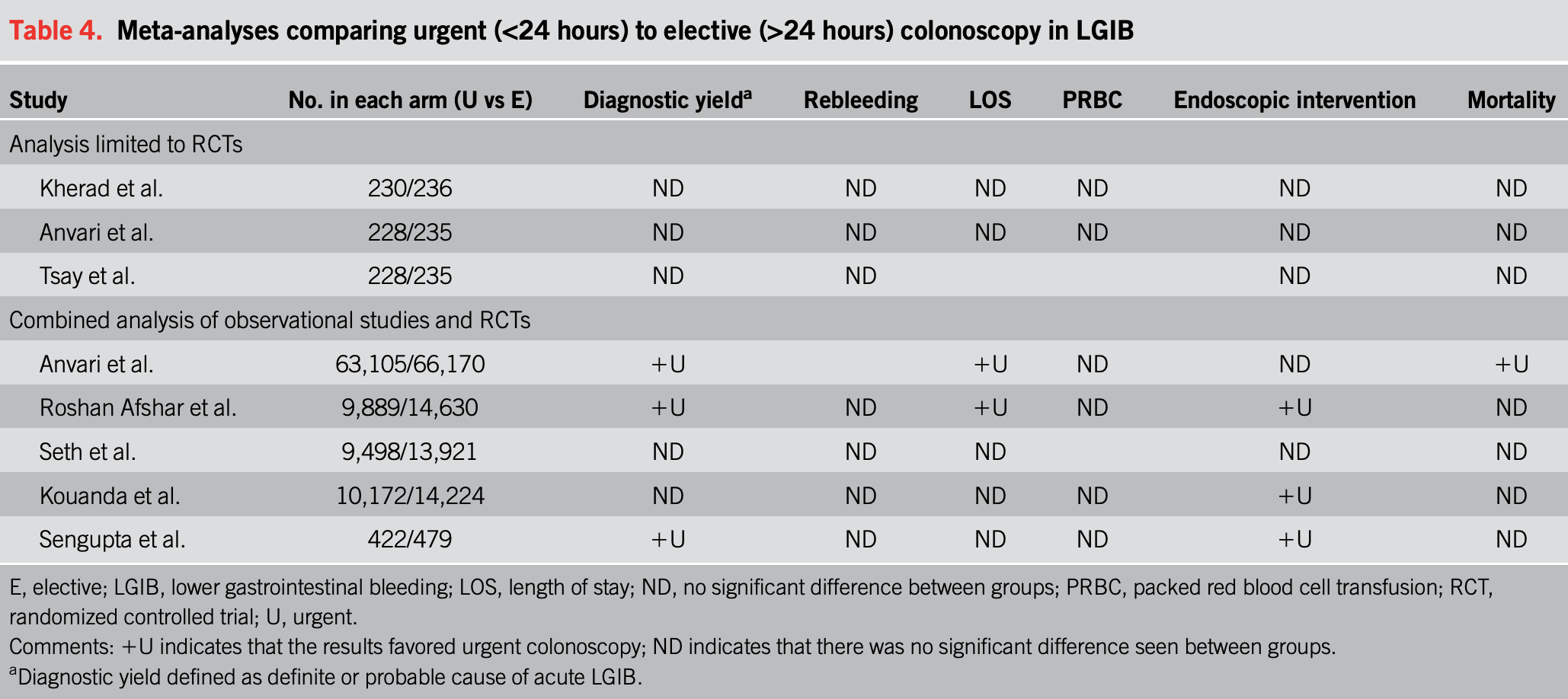
Recommendation: For patients hospitalized with LGIB requiring a colonoscopy, we recommend performing a nonemergent inpatient colonoscopy because performing an urgent colonoscopy within 24 hours has not been shown to improve clinical outcomes such as rebleeding and mortality. (Strong recommendation, moderate-quality evidence).
Role of treatment of stigmata of recent hemorrhage
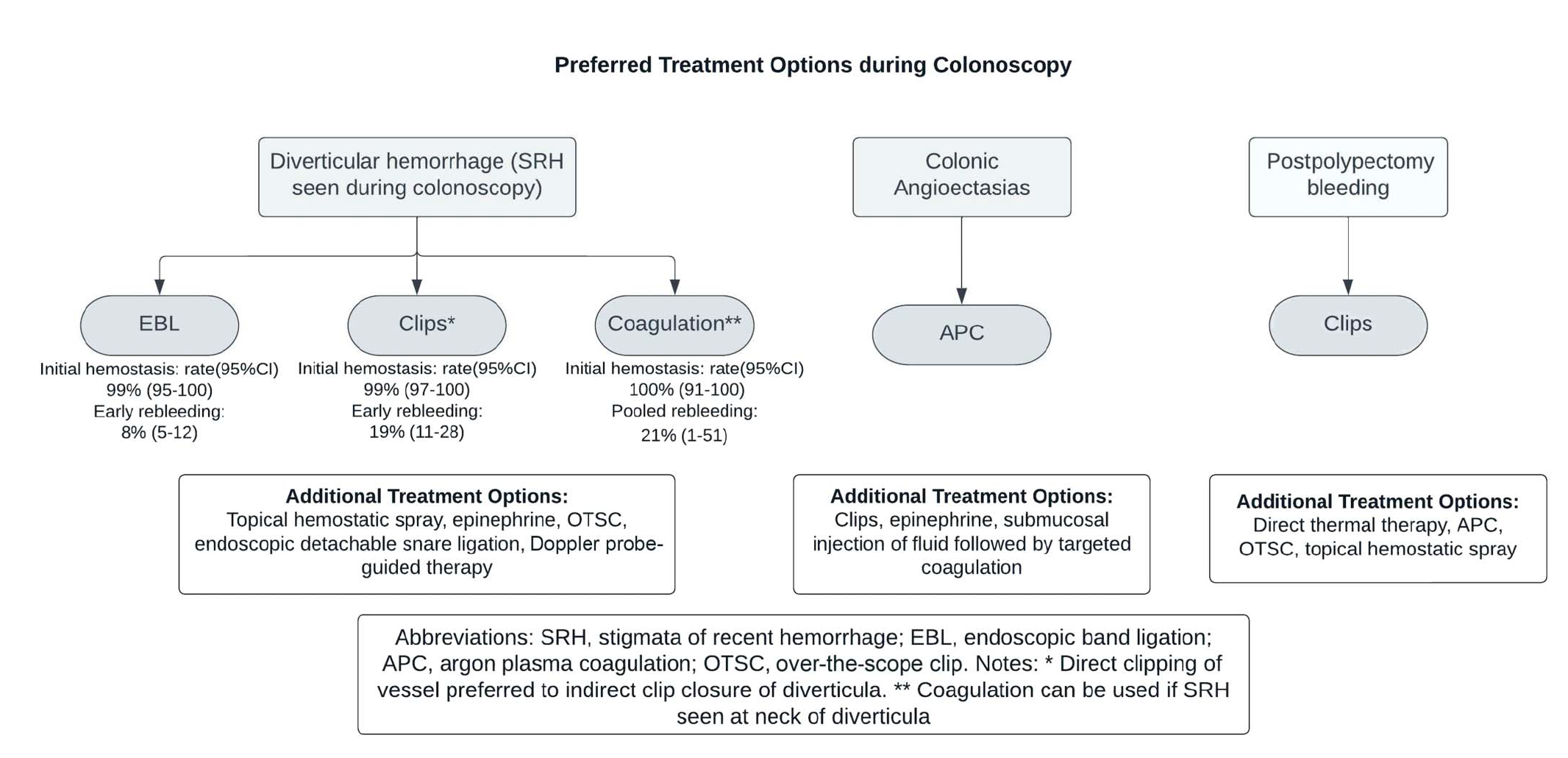
Key Concept: Endoscopic therapy is recommended when finding active bleeding or stigmata of recent hemorrhage (SRH), irrespective of the etiology.
Treatment of diverticular hemorrhage
Recommendation: When detected, we recommend treatment of diverticular SRH with through-the-scope clips, EBL, or coagulation. (Strong recommendation, moderate-quality evidence).
Role for repeat colonoscopy, angiography, and surgery
Key Concept: For patients experiencing rebleeding after initial hemostasis or cessation of bleeding, repeat colonoscopy can be considered depending on the patient’s stability and likelihood of successful repeat endoscopic therapy. In patients with suspected recurrent diverticular bleeding with recent colonoscopy who are hemodynamically stable, observation can be considered.
Resumption of antiplatelet medications and risk of recurrence
Recommendation: We recommend discontinuing nonaspirin NSAIDs after hospitalization for diverticular hemorrhage. (Strong recommendation, low-quality evidence).
Recommendation: We suggest discontinuing aspirin for primary cardiovascular prevention after hospitalization for diverticular hemorrhage given the risks of recurrent diverticular hemorrhage. (Conditional recommendation, low-quality evidence).
Recommendation: We suggest continuing aspirin after hospitalization for diverticular hemorrhage for patients with an established history of cardiovascular disease given the benefits of reducing future ischemic events. (Conditional recommendation, low-quality evidence).
Recommendation: We recommend that providers re-evaluate the risks vs benefits of continuing nonaspirin antiplatelets such as P2Y12 receptor antagonists in a multidisciplinary setting after hospitalization for diverticular hemorrhage given the demonstrated risks of recurrent diverticular hemorrhage. (Strong recommendation, low-quality evidence).
Resumption of anticoagulants and risk of recurrence
Recommendation: We recommend resuming anticoagulation after cessation of LGIB given that resumption of anticoagulation has been shown to decrease the risks of postbleeding thromboembolism and mortality. (Strong recommendation, moderate-quality evidence).
Algorithms: