
Author: Jacob Kirkland, MD (EM Resident Physician, UTSW – Dallas, TX); Stephen Field, DO (Assistant Professor of EM/Attending Physician, UTSW – Dallas, TX) // Reviewed by: Sophia Görgens, MD (EM Resident Physician, Zucker-Northwell NS/LIJ, NY); Cassandra Mackey, MD (Assistant Professor of Emergency Medicine, UMass Chan Medical School); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit)
Welcome to EM@3AM, an emDOCs series designed to foster your working knowledge by providing an expedited review of clinical basics. We’ll keep it short, while you keep that EM brain sharp.
A 32-year-old female with a history of hypertension and autoimmune hepatitis status post liver transplant 6 weeks prior on tacrolimus and mycophenolate presents to the ED with abdominal discomfort. For the past two days, she describes worsening pain and intermittent vomiting. She came today because her sister is a nurse who noticed her eyes were yellow. She denies fever or a new rash. She has been taking her medications as prescribed.
Vital signs: HR 118, BP 103/68, RR 20, T 99.8. On exam the patient is tachycardic with RUQ pain to palpation and scleral icterus. LFTs are in the thousands. A point of care ultrasound of the liver reveals the following:
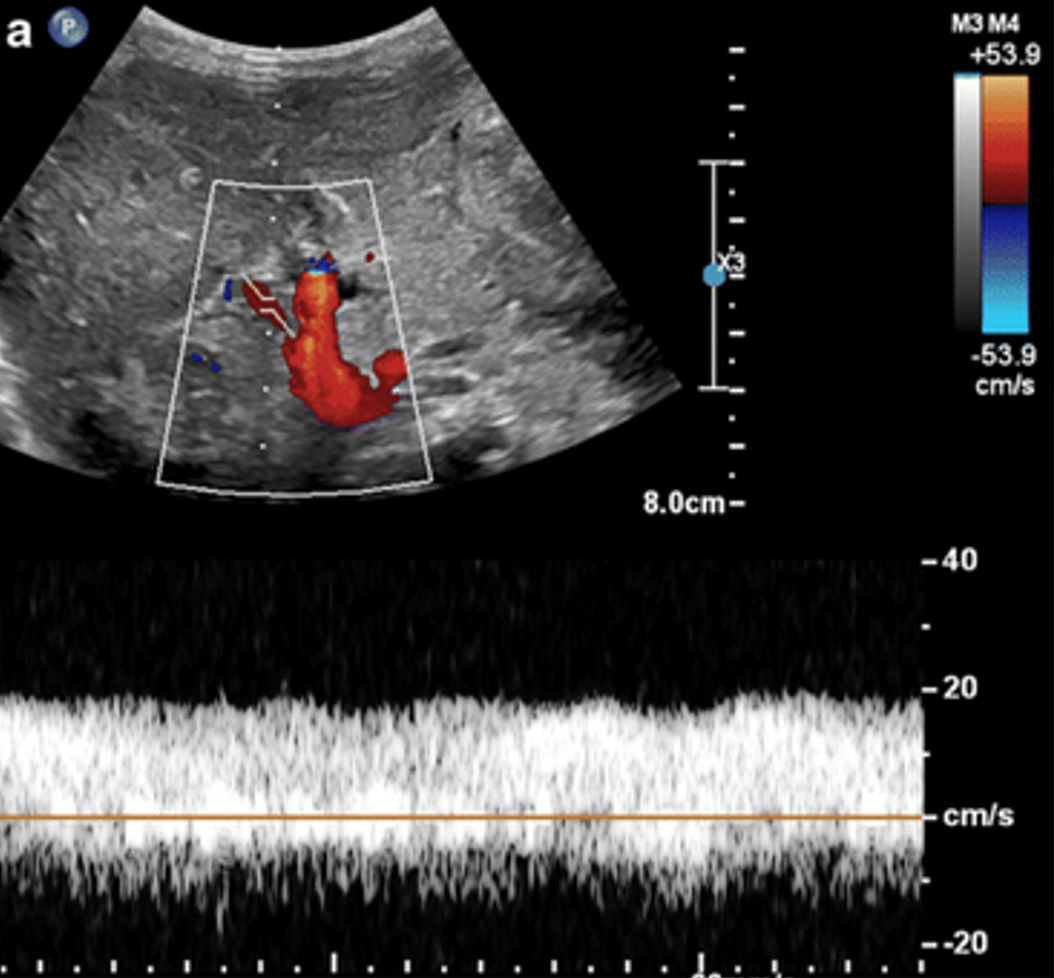
Image 1: Ultrasound of the liver showing abnormal hepatic artery flow and resistance index1
Question: What is the diagnosis? What are the complications of liver transplant that we see in the ED?
Answer: Hepatic artery thrombosis. Differential for liver complications post-transplant should include infection, organ rejection, transplant medication side effects, hepatic artery thrombosis or stenosis, and bile strictures, leaks, and bilomas.
Epidemiology
- There are ~100,000 living liver transplant patients as of 20202
- 2nd most common solid organ transplantation behind renal transplants
- 2020— 8907 transplants performed and 12,800 newly waitlisted patients
- 8,416 from deceased and 491 from alive persons
- Alcoholic liver disease is the most common cause for transplantation in US adults2
- Biliary atresia is the most common cause for transplantation in US children3
- One year survival post-transplant is approximately 93.6%2
- Highest mortality post-transplant attributed to infections4
- One study following liver transplant patients found that probability of ED visits and admissions were 43.6% and 49% at 1 year post op, respectively5
Anatomy

Image 2: Illustration of surgical anastomosis sites during liver transplant surgery6
- Donor liver takes place of diseased liver
- Surgical complications can occur at any site of anastomosis
- Anastomoses are used between the donor and recipient:
- Upper/lower IVC
- Hepatic artery
- Portal vein
- Biliary ducts
- Modifications include hepaticojejunostomy/choledochojejunostomy
Complications
- Complications specific to liver transplant patients as opposed to other types of transplants are typically mechanicaland related to vascular or biliary complications
- Vascular Complications
- Hepatic artery is the main blood supply to biliary epithelium
- Biliary ischemia will lead to bilomas, which are collections of bile outside of the biliary tree, strictures, and leaks7
- Hepatic artery thrombosis
- Early thrombosis period within approximately two months post-op7
- Incidence in adults approximately 4.4%, in children (8.3%)8
- Devastating effects with >50% requiring retransplant and >30% mortality9,10
- Presentation may display signs of fulminant liver failure
- Late thrombosis starts after one month and can be a more mild in presentation, can result with biliary complications11,12
- Doppler ultrasound will show absent/low flow in hepatic artery
- In early hepatic artery thrombosis within 7 days post-op, sensitivity reaches close to 100%10
- Sensitivity decreases over time or with late thrombosis
- Findings should be confirmed with contrast ultrasound or CTA
- Findings of CTA will show narrowing or occlusion of hepatic artery13
- Sensitivity upwards of 90%14
- Early thrombosis period within approximately two months post-op7
- Hepatic artery stenosis
- Presentation of stenosis is more similar to that of delayed thrombosis7
- Most common vascular complication post-op ranging from 5-13%11
- Doppler US has lower sensitivity at around 70% sensitivity showing high peak velocity15,16
- CTA may be needed if high index of suspicion or if doppler is inconclusive
- Hepatic pseudoaneurysm
- Incidence is rare–around 0.6-2.3%
- May be an incidental finding on imaging or present with severe intra-abdominal hemorrhage17
- US will show cystic structure arising from hepatic artery with disorganized flow on doppler18
- CTA will show increased contrast uptake in cyst-like structure15
- Hepatic artery is the main blood supply to biliary epithelium
- Biliary complications
- Biliary complications affect approximately 5-32% of liver transplant patients19
- Associated mortality ~10%20
- Commonly present with RUQ pain, sometimes with fever and pain15
- Clinically significant as these can lead to cholangitis, liver dysfunction, hyperbilirubinemia
- Doppler ultrasound has high positive predictive value in the presence of dilated biliary ducts, however has low sensitivity of 38%-66%15,19,21
- MRCP has a much higher sensitivity22 (96%) and specificity (94%) at detecting biliary complications15,23
- Strictures
- May be anastomotic (more common) or non-anastomotic which may be secondary to a vascular complication like hepatic artery thrombosis
- Stenting is treatment +/- ballooning7,24
- Bile Leaks
- Occur in up to 20% of transplants24
- Most commonly at anastomosis, can occur elsewhere with ischemia or obstruction7,24
- Bilious ascites should raise suspicion19
- Findings of biliary leakage seen on cholangiography MR/ERCP7,19
- Other complications include sphincter of oddi dysfunction and bilomas
- Biliary complications affect approximately 5-32% of liver transplant patients19
- Other common complications for transplant patients in general include:
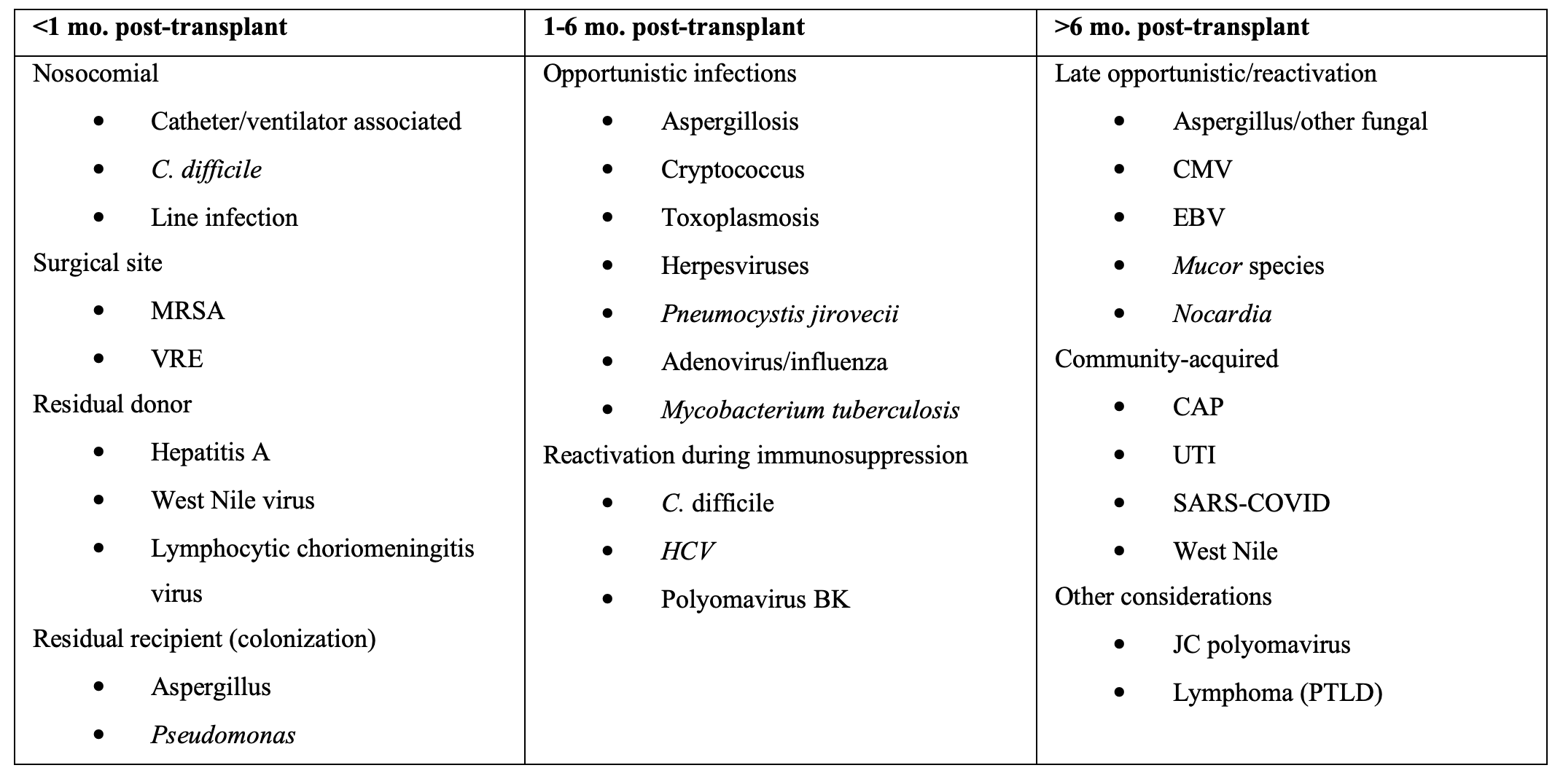
- Infection
- Primary cause of death in liver transplant patients25
- Nosocomial/surgical present <1month post-transplant
- Peak immunosuppression/opportunistic infections 1-6 months
- Community acquired generally >6 months15
- Primary cause of death in liver transplant patients25
- Infection
Table 1. Infections to Consider in Liver Transplant Patients15,26
- Rejection
- Allografted livers has a higher immunologic tolerance compared to other transplanted organs22
- Anti-inflammatory response to lipopolysaccharide, which exhausts active T-cells and generates regulatory T-cells
- Most commonly occurs within the first 90 days25
- May present similar to the above complications, however diagnosis made with liver biopsy26
- Ask if patient is compliant with taking medications, or if recent changes were made to immunosuppression therapy25
- Allografted livers has a higher immunologic tolerance compared to other transplanted organs22
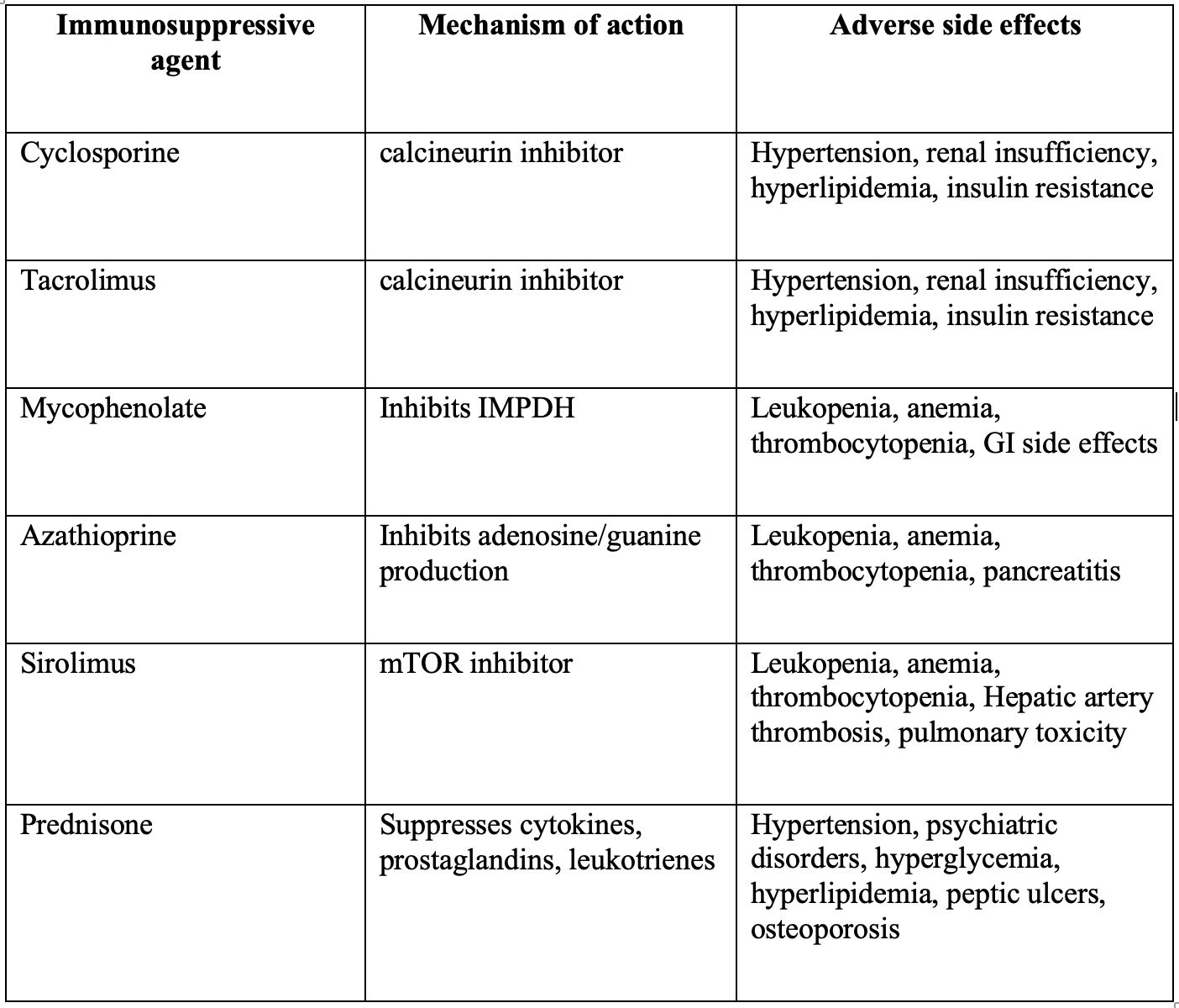
- Medication complications
- Consider patient’s immunosuppressive agents
- Side effects or medication interactions may be present
- Symptoms may range from renal dysfunction, anemia, metabolic syndrome, GI symptoms15,25
- Consider patient’s immunosuppressive agents
Table 2. Common Immunosuppressive Agents in Transplant patients15,25
Clinical Presentation
- A study of 290 liver transplant recipients revealed the most common presenting complaint to be GI related such as nausea, vomiting, or abdominal pain25,28
- 69% of these patients were hospitalized
- Symptoms of allograft dysfunction from above complications range from asymptomatic to severe cholangitis to fulminant liver failure
- Jaundice, dark urine, abdominal pain, pruritus, or fatigue may point towards allograft disfunction or rejection
Evaluation
- It is imperative to obtain a detailed history e.g. timing of transplant, prior complications
- Associated symptoms of allograft rejection include jaundice, fever, nausea, vomiting, diarrhea, abdominal pain, dark urine, edema25
- Laboratory testing should include at least CBC, CMP, INR25
- Look for elevated INR, elevated LFTs, thrombocytopenia, elevated bilirubin
- Other helpful tests depending on presentation include hepatitis panel, tacrolimus trough
- ESR/CRP have limited utility unless historically trended25
- Lack of fever does not rule out infection15,28
- Infection may present with leukocytosis or leukopenia
- Imaging
- Physicians should have a low threshold for imaging, especially with lab abnormalities
- Doppler US is helpful for detecting vascular/biliary complications
- Cons: user dependent, low sensitivity in some circumstances15,19,17
- CT with contrast or CTA have higher sensitivities7, 14
- Admitted patients may need MR/ERCP for definitive diagnosis
Treatment
- There should be a low threshold to contact patient’s transplant team
- Reduced dosages of acetaminophen may be used for pain control, granted the patient is not showing signs of live failure
- Opiates (fentanyl and hydromorphone preferred) may also be used for pain control, however reduce dosages/frequency to avoid accumulation
- Avoid NSAIDs, as patients on immunosuppressives are at high risk of AKI
- Cultures, broad spectrum antibiotics if concerned for systemic infection25
- Biliary/artery stenosis may need ERCP/stenting7
- Arterial thrombosis/stenosis may require IR/vascular surgery consultation25
- Bile leaks may require surgical consultation or stenting7
- Rejection may require IV methylprednisolone 500 to 1000 mg IV initial dose15
Disposition
- Liver transplant patients are at a high risk of admission23
- Early consultation with patient’s transplant surgery/hepatobiliary team
Pearls
- US is a great first line imaging tool for these patients, however CT may be necessary
- Contact the patient’s transplant/hepatobiliary team early in the ED course
- Perform a detailed history/exam, as allograft dysfunction has a broad range of symptoms
- Hepatic artery thrombosis is much more common in children, and has devastating consequences
- Allograft complications can occur at every site of anastomosis

A patient with hepatocellular carcinoma secondary to chronic hepatitis C infection underwent an orthotopic liver transplantation. He presents to the clinic reporting episodes of fever and abdominal pain 5 months later. A CT scan shows ductal dilation and a liver abscess. What is the most likely cause of this patient’s presentation?
A) Acute rejection
B) Biliary anastomosis stricture
C) Hepatic artery thrombosis
D) Portal vein thrombosis
Answer: C
This patient likely has a stricture of the common bile duct and liver abscesses. The blood supply to the common bile duct comes from the hepatic artery. Hepatic artery thrombosis is a dreaded complication of liver transplantation resulting in stricture of the duct. Although the liver has a dual blood supply with the portal vein and hepatic artery, thrombosis of the hepatic artery can result in hepatic parenchymal necrosis, which can later turn into an abscess. Hepatic artery thrombosis is managed conservatively with antibiotics for patients with bacteremia and percutaneous drainage for liver abscesses, but retransplantation is usually required.

Acute rejection (A) following liver transplant is uncommon and less likely than hepatic artery stenosis as the etiology of bile duct stricture and abscess formation. Biliary anastomosis stricture (B) as the result of a technical error is possible but will usually manifest immediately after surgery with obstructive cholangiopathy. Portal vein thrombosis (D) presents with signs and symptoms of portal hypertension, including encephalopathy and varices. It does not cause biliary stricture.
References
1) Karmazyn B, Sağlam D, Rao GS, Jennings SG, Mangus RS. Initial experience with contrast-enhanced ultrasound in the first week after liver transplantation in children: a useful adjunct to Doppler ultrasound. Pediatr Radiol. 2021;51(2):248-256. doi:10.1007/s00247-020-04811-0
2) Kwong AJ, Ebel NH, Kim WR, et al. OPTN/SRTR 2020 Annual Data Report: Liver. Am J Transplant. 2022;22 Suppl 2:204-309. doi:10.1111/ajt.16978
3) Miyara SJ, Sardo Molmenti CL, Guevara S, Hayashida K, Shinozaki K, Zafeiropoulos S, Becker LB. Epidemiology of Liver Transplantation. In: Molmenti E, Santibañes M, Santibañes E. eds. Liver Transplantation: Operative Techniques and Medical Management. McGraw Hill; 2021. Accessed April 21, 2023. https://accesssurgery.mhmedical.com/content.aspx?bookid=3006§ionid=253170962
4) Gaglio, PJ, Brown RS, Robson KM. Liver transplantation in adults: Long-term management of transplant recipients. In: Post T, ed. UpToDate. Waltham, Mass.: UpToDate; 2023. www.uptodate.com. Accessed May 7, 2023
5) Oh SY, Lee JM, Lee H, et al. Emergency department visits and unanticipated readmissions after liver transplantation: A retrospective observational study. Sci Rep. 2018;8(1):4084. Published 2018 Mar 6. doi:10.1038/s41598-018-22404-8
6) Vilarinho S, Lifton RP. Liver transplantation: from inception to clinical practice. Cell. 2012;150(6):1096-1099. doi:10.1016/j.cell.2012.08.030
7) Brookmeyer CE, Bhatt S, Fishman EK, Sheth S. Multimodality Imaging after Liver Transplant: Top 10 Important Complications. Radiographics. 2022;42(3):702-721. doi:10.1148/rg.210108
8) Bekker J, Ploem S, de Jong KP. Early hepatic artery thrombosis after liver transplantation: a systematic review of the incidence, outcome and risk factors. Am J Transplant. 2009;9(4):746-757. doi:10.1111/j.1600-6143.2008.02541.x
9) Horrow MM, Blumenthal BM, Reich DJ, Manzarbeitia C. Sonographic diagnosis and outcome of hepatic artery thrombosis after orthotopic liver transplantation in adults. AJR Am J Roentgenol. 2007;189(2):346-351. doi:10.2214/AJR.07.2217
10) Bastón Castiñeiras M, Benítez Linero I, Serrano Zarcero V, Fernández Castellano G, Suárez-Artacho G, López Romero JL. Hepatic Artery Thrombosis After Orthotopic Liver Transplant: Experience in the Last 10 Years. Transplant Proc. 2022;54(1):51-53. doi:10.1016/j.transproceed.2021.11.006
11) Frongillo F, Lirosi MC, Nure E, et al. Diagnosis and Management of Hepatic Artery Complications After Liver Transplantation. Transplant Proc. 2015;47(7):2150-2155. doi:10.1016/j.transproceed.2014.11.068
12) Valente JF, Alonso MH, Weber FL, Hanto DW. Late hepatic artery thrombosis in liver allograft recipients is associated with intrahepatic biliary necrosis. Transplantation. 1996;61(1):61-65. doi:10.1097/00007890-199601150-00013
13)Baheti AD, Sanyal R, Heller MT, Bhargava P. Surgical Techniques and Imaging Complications of Liver Transplant. Radiol Clin North Am. 2016;54(2):199-215. doi:10.1016/j.rcl.2015.09.004
14) Kim JS, Kim DW, Kim KW, Song GW, Lee SG. Improving the Specificity of CT Angiography for the Diagnosis of Hepatic Artery Occlusion after Liver Transplantation in Suspected Patients with Doppler Ultrasound Abnormalities. Korean J Radiol. 2022;23(1):52-59. doi:10.3348/kjr.2021.0266
15) Long B, Koyfman A. The emergency medicine approach to transplant complications. Am J Emerg Med. 2016;34(11):2200-2208. doi:10.1016/j.ajem.2016.08.049
16) Orons PD, Zajko AB. Angiography and interventional procedures in liver transplantation. Radiol Clin North Am. 1995;33(3):541-558.
17) St Michel DP, Goussous N, Orr NL, et al. Hepatic Artery Pseudoaneurysm in the Liver Transplant Recipient: A Case Series. Case Rep Transplant. 2019;2019:9108903. Published 2019 Dec 27. doi:10.1155/2019/9108903
18) Fang A, Ashwani K. Sharma, Rubens D. Hepatic Artery After Liver Transplant: Ultrasonographic Diagnosis for Intervention. Ultrasound Clinics. 2013;8(2):249-258. doi:10.1016/j.cult.2012.12.009.
19) Kochhar G, Parungao JM, Hanouneh IA, Parsi MA. Biliary complications following liver transplantation. World J Gastroenterol. 2013;19(19):2841-2846. doi:10.3748/wjg.v19.i19.2841
20) Moy BT, Birk JW. A Review on the Management of Biliary Complications after Orthotopic Liver Transplantation. J Clin Transl Hepatol. 2019;7(1):61-71. doi:10.14218/JCTH.2018.00028
21)Verdonk RC, Buis CI, Porte RJ, et al. Anastomotic biliary strictures after liver transplantation: causes and consequences. Liver Transpl. 2006;12(5):726-735. doi:10.1002/lt.20714
22) Kitazono MT, Qayyum A, Yeh BM, Chard PS, Ostroff JW, Coakley FV. Magnetic resonance cholangiography of biliary strictures after liver transplantation: a prospective double-blind study. J Magn Reson Imaging. 2007;25(6):1168-1173. doi:10.1002/jmri.20927
23) Jorgensen JE, Waljee AK, Volk ML, et al. Is MRCP equivalent to ERCP for diagnosing biliary obstruction in orthotopic liver transplant recipients? A meta-analysis. Gastrointest Endosc. 2011;73(5):955-962. doi:10.1016/j.gie.2010.12.014
24) Senter-Zapata M, Khan AS, Subramanian T, et al. Patient and Graft Survival: Biliary Complications after Liver Transplantation. J Am Coll Surg. 2018;226(4):484-494. doi:10.1016/j.jamcollsurg.2017.12.039
25) Rayan El Sibai, Sari R. Freedman, J. David Gatz, A narrative review of the evaluation and management of liver transplant complications in the emergency department. The Journal of Emergency Medicine. 2023; https://doi.org/10.1016/j.jemermed.2023.02.022.
26) Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med. 2007;357(25):2601-2614. doi:10.1056/NEJMra064928
27) Taner T. Liver transplantation: Rejection and tolerance. Liver Transpl. 2017;23(S1):S85-S88. doi:10.1002/lt.24840
28) Savitsky EA, Votey SR, Mebust DP, Schwartz E, Uner AB, McCain S. A descriptive analysis of 290 liver transplant patient visits to an emergency department. Acad Emerg Med. 2000;7(8):898-905. doi:10.1111/j.1553-2712.2000.tb02068.x





{kind=link}